Come the year 2012 there could be a new antidepressant with a novel mechanism of action on the market in these United States (1). As the drug is still in development, it is known as "TC-5214."
According the the press release, TC-5214 is a "nicotinic channel blocker that is thought to treat depression by acting on neuronal nicotinic receptors, or NNRs, according to Targacept. Targacept says NNRs are found on nerve cells throughout the nervous system and regulate nervous system activity."
The Cholinergic Hypothesis of Depression?
среда, 23 декабря 2009 г.
Zicronapine
Zicronapine shows significant positive data in clinical phase II in the treatment of patients with schizophrenia - planning for continued clinical work
Corporate Release No 392
18 December 2009
H. Lundbeck A/S (Lundbeck) today announced strongly positive headline results
from the clinical trials in the phase II development programme with zicronapine
in schizophrenia. The programme consisted of two studies which in total involved
approximately 375 patients.
In the two recently completed randomised clinical phase II trials, zicronapine
was tested in several dosages between 3-10 mg/day. The two studies were
exploratory and therefore not powered to show clear statistical differences.
However, in the studies zicronapine did show clear statistical significant
separation from placebo at 7 and 10 mg and very convincing efficacy and safety
data when compared to olanzapine justifying further development.
In the placebo-controlled trial, zicronapine showed clear dose-response and a
statistically significant improvement in PANSS score on both 7 and 10 mg. In the
olanzapine-referenced study, zicronapine showed comparable reduction in PANSS
score.
From both trials it can be concluded that zicronapine was safe and
well-tolerated. In the olanzapine-referenced study the number of withdrawals was
similar to the level of withdrawals in the olanzapine-group.
"We are pleased to see the efficacy and supportive data enabling us to continue
the development program," says Executive Vice President Anders Gersel Pedersen,
Head of Drug Development at Lundbeck. "We are also pleased that the good safety
profile seen in earlier studies now is confirmed in a much larger patient
population.?
In the coming months, Lundbeck will finalise the planning for additional
clinical work including plans for the pivotal programme.
About the study
In the placebo-controlled clinical phase II study approximately 280 patients
from 11 countries suffering from schizophrenia were enrolled. Eligible patients
have been randomised in a 2:1 ratio to blinded treatment with either zicronapine
(3, 5, 7 and 10 mg/day) or placebo for 8 weeks. The primary focus of this trial
was safety and tolerability measured by adverse events, clinical safety
laboratory tests and metabolic parameters. Secondary outcome measures included
Positive and Negative Syndrome Scale (PANSS) and Clinical Global Impression ?
Severity/Improvement (CGI-S/I) scores.
In the second clinical phase II study approximately 93 patients were enrolled
from nine countries. Eligible patients were randomised to treatment with either
flexible doses (5-7 mg/day) of zicronapine or flexible doses of olanzapine
(10-15 mg/day) for 12 weeks. The efficacy and the safety of zicronapine were
explored in comparison to olanzapine. The primary outcome measures included the
PANSS score. Secondary outcome measures included CGI-S/I and Calgary Depression
Scale for Schizophrenia (CDSS) scores.
About zicronapine (previously known as Lu 31-130)
Zicronapine has a multi-receptorial profile. In vitro and in vivo, zicronapine
has shown potent antagonistic effects at dopamine D(1), D(2) and 5-HT(2a)
receptors. Based on the profile from antipsychotic animal models, zicronapine
was expected to show clear and convincing effects in patients with schizophrenia
and likely associated with low potential for neurological side effects and a
benign safety/tolerability profile.
schizophrenia.com
Corporate Release No 392
18 December 2009
H. Lundbeck A/S (Lundbeck) today announced strongly positive headline results
from the clinical trials in the phase II development programme with zicronapine
in schizophrenia. The programme consisted of two studies which in total involved
approximately 375 patients.
In the two recently completed randomised clinical phase II trials, zicronapine
was tested in several dosages between 3-10 mg/day. The two studies were
exploratory and therefore not powered to show clear statistical differences.
However, in the studies zicronapine did show clear statistical significant
separation from placebo at 7 and 10 mg and very convincing efficacy and safety
data when compared to olanzapine justifying further development.
In the placebo-controlled trial, zicronapine showed clear dose-response and a
statistically significant improvement in PANSS score on both 7 and 10 mg. In the
olanzapine-referenced study, zicronapine showed comparable reduction in PANSS
score.
From both trials it can be concluded that zicronapine was safe and
well-tolerated. In the olanzapine-referenced study the number of withdrawals was
similar to the level of withdrawals in the olanzapine-group.
"We are pleased to see the efficacy and supportive data enabling us to continue
the development program," says Executive Vice President Anders Gersel Pedersen,
Head of Drug Development at Lundbeck. "We are also pleased that the good safety
profile seen in earlier studies now is confirmed in a much larger patient
population.?
In the coming months, Lundbeck will finalise the planning for additional
clinical work including plans for the pivotal programme.
About the study
In the placebo-controlled clinical phase II study approximately 280 patients
from 11 countries suffering from schizophrenia were enrolled. Eligible patients
have been randomised in a 2:1 ratio to blinded treatment with either zicronapine
(3, 5, 7 and 10 mg/day) or placebo for 8 weeks. The primary focus of this trial
was safety and tolerability measured by adverse events, clinical safety
laboratory tests and metabolic parameters. Secondary outcome measures included
Positive and Negative Syndrome Scale (PANSS) and Clinical Global Impression ?
Severity/Improvement (CGI-S/I) scores.
In the second clinical phase II study approximately 93 patients were enrolled
from nine countries. Eligible patients were randomised to treatment with either
flexible doses (5-7 mg/day) of zicronapine or flexible doses of olanzapine
(10-15 mg/day) for 12 weeks. The efficacy and the safety of zicronapine were
explored in comparison to olanzapine. The primary outcome measures included the
PANSS score. Secondary outcome measures included CGI-S/I and Calgary Depression
Scale for Schizophrenia (CDSS) scores.
About zicronapine (previously known as Lu 31-130)
Zicronapine has a multi-receptorial profile. In vitro and in vivo, zicronapine
has shown potent antagonistic effects at dopamine D(1), D(2) and 5-HT(2a)
receptors. Based on the profile from antipsychotic animal models, zicronapine
was expected to show clear and convincing effects in patients with schizophrenia
and likely associated with low potential for neurological side effects and a
benign safety/tolerability profile.
schizophrenia.com
вторник, 22 декабря 2009 г.
SNRIs Anti-depressants
Trazodone (Desyrel) inhibits serotonin reuptake in addition to blocking certain types of serotonin, norepinephrine, and histamine receptors. Histamine is a both a biological chemical involved in immune responses as well as a neurotransmitter. In low doses, Trazodone can be used as a sleep aid, especially for people who experience insomnia as part of their depression. Side effects of Trazodone include: allergic reactions, irregular heartbeat, prolonged and painful erection, drowsiness, fatigue, lethargy (exhaustion), psychomotor retardation (slow movements), lightheadedness, dizziness, difficulty concentrating, confusion, impaired memory, disorientation, excitement, agitation, anxiety, tension, nervousness, restlessness, insomnia, nightmares, anger, hostility and, rarely, hypomania, visual distortions, hallucinations (sensing things that aren't really there), delusions (false, fixed beliefs), and paranoia (suspicious fear).
Buproprion (Wellbutrin) is often a first choice treatment for Major Depressive Disorder. This medication is just as effective as SSRIs in treating depressive symptoms, with less risk of weight gain and sexual side effects. In addition to serotonin and norepinephrine, buproprion also inhibits dopamine reuptake. The most common side effects of buproprion are dry mouth, constipation, headaches, and insomnia. Care must be taken when using buproprion at higher doses, as it has been known to cause seizures.
Venlafaxine (Effexor) is often used for the treatment of depressive illnesses, but large numbers of studies demonstrating treatment success are lacking. In addition to inhibiting serotonin reuptake, venlafaxine inhibits norepinephrine and dopamine reuptake. Venlafaxine does not interfere with other brain chemicals, which makes it less "messy" and more powerful than other antidepressants. Some evidence suggests that venlafaxine relieves depressive symptoms more quickly than other medications with fewer side effects, and that it can be combined safely with other medications. However, more research is necessary to substantiate these claims.
Nefazodone (Serzone) inhibits serotonin reuptake by blocking a particular type of serotonin receptor. Serzone is sedating, and is useful for relieving anxiety and severe insomnia. Furthermore, sexual side effects are mild, if any. Unfortunately however, nefazodone is a strong inhibitor of liver enzymes and should be used cautiously. Many medications are metabolized in the liver, and functional liver enzymes are essential to proper liver functioning and overall health.
Mirtazapine (Remeron) blocks serotonin and norepinephrine reuptake. Mirtazapine is sedating, and has the disagreeable side effect (for most) of weight gain in comparison with other SSRIs. Although few studies clearly demonstrate Mirtazapine's usefulness in treating unipolar depression, this medication may be a good option for people who have experienced significant weight loss during their depressive episodes.
Antidepressants for Major Depression - Selective Serotonin and Norepinephrine Reuptake Inhibitors (SNRI)
Trazodone (Desyrel) inhibits serotonin reuptake in addition to blocking certain types of serotonin, norepinephrine, and histamine receptors. Histamine is a both a biological chemical involved in immune responses as well as a neurotransmitter. In low doses, Trazodone can be used as a sleep aid, especially for people who experience insomnia as part of their depression. Side effects of Trazodone include: allergic reactions, irregular heartbeat, prolonged and painful erection, drowsiness, fatigue, lethargy (exhaustion), psychomotor retardation (slow movements), lightheadedness, dizziness, difficulty concentrating, confusion, impaired memory, disorientation, excitement, agitation, anxiety, tension, nervousness, restlessness, insomnia, nightmares, anger, hostility and, rarely, hypomania, visual distortions, hallucinations (sensing things that aren't really there), delusions (false, fixed beliefs), and paranoia (suspicious fear).
Buproprion (Wellbutrin) is often a first choice treatment for Major Depressive Disorder. This medication is just as effective as SSRIs in treating depressive symptoms, with less risk of weight gain and sexual side effects. In addition to serotonin and norepinephrine, buproprion also inhibits dopamine reuptake. The most common side effects of buproprion are dry mouth, constipation, headaches, and insomnia. Care must be taken when using buproprion at higher doses, as it has been known to cause seizures.
Venlafaxine (Effexor) is often used for the treatment of depressive illnesses, but large numbers of studies demonstrating treatment success are lacking. In addition to inhibiting serotonin reuptake, venlafaxine inhibits norepinephrine and dopamine reuptake. Venlafaxine does not interfere with other brain chemicals, which makes it less "messy" and more powerful than other antidepressants. Some evidence suggests that venlafaxine relieves depressive symptoms more quickly than other medications with fewer side effects, and that it can be combined safely with other medications. However, more research is necessary to substantiate these claims.
Nefazodone (Serzone) inhibits serotonin reuptake by blocking a particular type of serotonin receptor. Serzone is sedating, and is useful for relieving anxiety and severe insomnia. Furthermore, sexual side effects are mild, if any. Unfortunately however, nefazodone is a strong inhibitor of liver enzymes and should be used cautiously. Many medications are metabolized in the liver, and functional liver enzymes are essential to proper liver functioning and overall health.
Mirtazapine (Remeron) blocks serotonin and norepinephrine reuptake. Mirtazapine is sedating, and has the disagreeable side effect (for most) of weight gain in comparison with other SSRIs. Although few studies clearly demonstrate Mirtazapine's usefulness in treating unipolar depression, this medication may be a good option for people who have experienced significant weight loss during their depressive episodes.
Antidepressants for Major Depression - Selective Serotonin and Norepinephrine Reuptake Inhibitors (SNRI)

"Why does this matter? Because the two scales used to rate depression in this study, the Hamilton Scale and the Montgomery-Asberg Scale, both count reduced appetite and sleeplessness as symptoms of depression. If you're on mirtazapine, you're unlikely to have either problem - you'll be more worried about the exact opposite, insatiable hunger and drowsiness. So mirtazapine could reduce your total score on these scales even if it didn't change your mood. I have no idea to what extent this is a factor in these results, but it could be important."
Two Drugs Are Better Than One?
четверг, 17 декабря 2009 г.
ранний ответ на терапию как предиктор эффективности лечения рисперидоном
Our objective was to prospectively assess whether early (ie, 2 weeks) response to an antipsychotic predicts later (12-week) response and whether ‘switching’ early non-responders to another antipsychotic is a better strategy than ‘staying’.
This is the first study to prospectively show that early response/non-response to an antipsychotic (risperidone) is a reliable clinical marker of subsequent clinical outcomes and that a ‘switching’ strategy based on this information may lead to greater clinical improvement than staying on a drug for a longer period in some patients.
Early Response to Antipsychotic Drug Therapy as a Clinical Marker of Subsequent Response in the Treatment of Schizophrenia
This is the first study to prospectively show that early response/non-response to an antipsychotic (risperidone) is a reliable clinical marker of subsequent clinical outcomes and that a ‘switching’ strategy based on this information may lead to greater clinical improvement than staying on a drug for a longer period in some patients.
Early Response to Antipsychotic Drug Therapy as a Clinical Marker of Subsequent Response in the Treatment of Schizophrenia
понедельник, 14 декабря 2009 г.
сравнение высоких и низких доз кветиапина в терапии шизофрении
BACKGROUND: Quetiapine fumarate (Seroquel [ICI 204,636]) is an atypical dibenzothiazepine antipsychotic with a greater affinity for 5-hydroxytryptamine2 (5-HT2) receptors than for D2 dopamine receptors; its efficacy in patients with schizophrenia was shown in early phase 2 trials (maximum dose, 750 mg/d). METHODS: In this multicenter, double-blind, placebo-controlled trial, 286 patients hospitalized with chronic or subchronic schizophrenia (DSM-III-R) were randomized to 6 weeks of treatment with high-dose quetiapine fumarate (< or = 750 mg/d), n = 96; low-dose quetiapine fumarate (< or = 250 mg/d), n = 94; or placebo, n = 96. The Brief Psychiatric Rating Scale (BPRS) and Clinical Global Impression Severity of Illness item scores were the primary efficacy variables. Secondary efficacy variables included the BPRS positive-symptom cluster score, the Modified Scale for the Assessment of Negative Symptoms summary score (United States only), and the total score from the negative scale of the Positive and Negative Syndrome Scale (Europe only). Scores were analyzed using an analysis of covariance for change from baseline at end point with last observations carried forward. The model included baseline score (covariate), center, and treatment. Extrapyramidal symptoms were assessed using the Simpson-Angus Scale and the Barnes Akathisia Scale; abnormal involuntary movements were assessed using the Abnormal Involuntary Movement Scale. Frequency distributions of grouped change-from-baseline scores were analyzed using chi 2 tests. RESULTS: Of 280 patients in whom the efficacy of quetiapine was evaluated, 159 (42% of those receiving high-dose treatment; 57%, low-dose treatment; and 59%, placebo) withdrew before trial completion, primarily because of treatment failure. Significant (P < .001, BPRS; P = .003, Clinical Global Impression Severity of Illness item; and P = .003, BPRS positive-symptom cluster) differences were identified between patients receiving high-dose quetiapine and placebo for both primary efficacy variables, with end point differences in the BPRS positive-symptom cluster score showing quetiapine's consistency in reducing positive symptoms. The reduction of negative symptoms was less consistent; high-dose quetiapine was superior on the Modified Scale for the Assessment of Negative Symptoms but not on the negative scale of the Positive and Negative Syndrome Scale. Quetiapine was well tolerated and did not induce extrapyramidal symptoms, sustained elevations of prolactin, or clinically significant changes in hematologic parameters. CONCLUSIONS: Quetiapine is an effective antipsychotic with a favorable safety profile. The optimum dose is probably greater than 250 mg/d.
Quetiapine in patients with schizophrenia. A high- and low-dose double-blind comparison with placebo. Seroquel Study Group.
Quetiapine in patients with schizophrenia. A high- and low-dose double-blind comparison with placebo. Seroquel Study Group.
коррекция акатизии вызванной нейролептиками при помощи пиридоксина
his study was conducted in 2 mental health centers from February 2003 to November 2003. Twenty schizophrenia and schizoaffective inpatients with a DSM-IV diagnosis of NIA were randomly divided to receive vitamin B6 600 mg/day b.i.d. (N = 10) or placebo (N = 10) twice a day for 5 days in a double-blind design.
The vitamin B6-treated patients in comparison with the placebo group showed a significant improvement on the subjective-awareness of restlessness (p = .0004), subjective-distress (p = .01), and global (p = .004) subscales of the BAS. The objective subscale did not demonstrate significant positive results (p = .079), but there was a trend of symptom amelioration in the vitamin B6 group. A reduction of at least 2 points on the BAS global subscale was noted in 8 patients in the vitamin B6 group (80%), and in only 3 patients in the placebo group (30%) (p = .037).
Vitamin B6 Treatment in Acute Neuroleptic-Induced Akathisia: A Randomized, Double-Blind, Placebo-Controlled Study.
The vitamin B6-treated patients in comparison with the placebo group showed a significant improvement on the subjective-awareness of restlessness (p = .0004), subjective-distress (p = .01), and global (p = .004) subscales of the BAS. The objective subscale did not demonstrate significant positive results (p = .079), but there was a trend of symptom amelioration in the vitamin B6 group. A reduction of at least 2 points on the BAS global subscale was noted in 8 patients in the vitamin B6 group (80%), and in only 3 patients in the placebo group (30%) (p = .037).
Vitamin B6 Treatment in Acute Neuroleptic-Induced Akathisia: A Randomized, Double-Blind, Placebo-Controlled Study.
пятница, 11 декабря 2009 г.
среда, 9 декабря 2009 г.
вторник, 8 декабря 2009 г.

понедельник, 7 декабря 2009 г.

пятница, 4 декабря 2009 г.

депривация сна
Ms. W’s chronotherapy protocol: Hours permitted for sleep*
Day number | |||||
| 1 | 2 | 3 | 4 | 5 |
Sleep deprivation | 9 PM to2 AM |
|
|
|
|
Sleep-phase advance |
| 5 PM to midnight | 7 PM to 2 AM | 9 PM to 4 AM | 10 PM to 5 AM |
*Treatment was implemented while Ms. W was hospitalized | |||||
The bedtime solution
понедельник, 30 ноября 2009 г.
потенциирование клозапина метадоном в терапии резистентной к лечению шизофрении без героиновой зависимости
We postulate a possible mechanism that might explain our patient's response. It is
possible that methadone could have acted synergically with clozapine at glutamate NMDA receptor(NMDAR) site. Clozapine and methadone are, respectively, agonist and antagonists at NMDAR site 4, 5. We think that the interaction of clozapine and methadone at NMDAR site might explain our patient's improvement, according to Shim and
colleagues' hypothesis [4]. They hypothesise that an ideal set-point of NMDAR stimulation is needed to achieve symptomatic remission. Our hypothesis is that methadone (an NMDAR antagonist)in association with clozapine (NMDAR agonist)
Methadone augmentation of clozapine in treatment-resistant schizophrenia without opiates addiction: a case report.
possible that methadone could have acted synergically with clozapine at glutamate NMDA receptor(NMDAR) site. Clozapine and methadone are, respectively, agonist and antagonists at NMDAR site 4, 5. We think that the interaction of clozapine and methadone at NMDAR site might explain our patient's improvement, according to Shim and
colleagues' hypothesis [4]. They hypothesise that an ideal set-point of NMDAR stimulation is needed to achieve symptomatic remission. Our hypothesis is that methadone (an NMDAR antagonist)in association with clozapine (NMDAR agonist)
Methadone augmentation of clozapine in treatment-resistant schizophrenia without opiates addiction: a case report.
пятница, 27 ноября 2009 г.
SeCA-депрессия
Тревога, сниженный фон настроения, (ауто)агрессивность часто взаимосвязаны, так же как и нозологические категории расстройств настроения и тревожных расстройств. Вследствие этого возникают сложности и в клинической практике, и в исследовательской работе. В клинике перед врачом встают вопросы: какие симптомы или расстройства надо лечить? Надо ли лечить все? В исследовательской работе - какие симптомы или расстройства коррелирует с полученными данными? Для решения этих проблем предложено два подхода: правила иерархического исключения и комбинированные диагнозы. Применение первого подхода является не вполне адекватным, так как ни одна проблема не может быть решена путем ее исключения. Второй подход, связанным с применением комбинированного диагноза, к примеру, атипичная депрессия, или смешанные тревожно-депрессивные расстройства, также не вполне правомочен. Предложенная нами недавно концепция “тревожно-агрессивной депрессии, провоцируемой стрессом, индуцируемой кортизолом и связанной с серотонином” (СеТА депрессии) определяет (пока гипотетически) подтип депрессии, при которой неконтролируемую чувства тревоги и агрессивность предшествуют и задают ритм снижению настроения. Повышенная ранимость, обусловленная невротическими особенностями личности, предрасполагает к возникновению СеТАдепрессии. В основе ее развития от психотравмирующих переживаний к психопатологии - сначала тревоги и агрессивности, а затем депрессии — лежит нарушение функции опальной связи между серотонинергической и гипоталамо-гипофизарно-адренокортикальной системами.
Депрессия, тревожные расстройства, агрессия: попытки распутать гордиев узел
Депрессия, тревожные расстройства, агрессия: попытки распутать гордиев узел
четверг, 26 ноября 2009 г.
Микседематозная кома вызванная комбинацией арипипразола и сертралина
Myxedema Coma Associated with Combination Aripiprazole and Sertraline Therapy
Chelsea O Church, PharmD BCPS
Associate Professor of Pharmacy Practice, College of Pharmacy, Southwestern Oklahoma State University, Weatherford, OK
Erin C Callen, PharmD BCPS
Associate Professor of Pharmacy Practice, College of Pharmacy, Southwestern Oklahoma State University
Reprints: Dr. Church, Department of Pharmacy Practice, Southwestern Oklahoma State University College of Pharmacy, Pasteur Medical Building, Pharmacy Education, 1111 North Lee, Ste. 241, Oklahoma City, OK 73103, fax 405/601-1201, chelsea.church@swosu.edu
OBJECTIVE: To describe a case of myxedema coma (MC) associated with combination aripiprazole and sertraline therapy.
CASE SUMMARY: A 41-year-old male presented to the emergency department with confusion, right-sided numbness and tingling, slurred speech, dizziness, and facial edema. His blood pressure was 160/113 mm Hg, with a pulse of 56 beats/min and temperature of 35.4 °C. Initial abnormal laboratory values included creatine kinase (CK) 439 U/L; serum creatinine 1.6 mg/dL; aspartate aminotransferase 85 U/L; and alanine aminotransferase 35 U/L. Repeat cardiac markers revealed an elevated CK level of 3573 U/L with a CK-MB of 24 ng/mL. Thyroid function tests showed thyroid-stimulating hormone 126.4 µIU/mL and free thyroxine 0.29 ng/dL. Home medications of unknown duration were sertraline 200 mg and aripiprazole 20 mg daily. He was admitted to the intensive care unit and initially treated with intravenous levothyroxine and dexamethasone. By hospital day 4, the patient was clinically stable and discharged to home.
DISCUSSION: Myxedema coma, the most significant form of hypothyroidism (HT), is a rare but potentially fatal condition. The known precipitating causes of MC were ruled out in this patient, which left his home medications as the likely cause. Cases of HT caused by certain atypical antipsychotics and antidepressants are found in the literature, but none was reported with aripiprazole therapy. There are also no reported cases of sertraline or aripiprazole inducing MC. Use of the Naranjo probability scale indicates that the combination of aripiprazole and sertraline was a probable inducer of MC in this patient.
CONCLUSIONS: Due to the widespread use of psychotropic medications, clinicians should be reminded of the rare, yet life-threatening, occurrence of MC when treating patients, especially with combination therapies such as sertraline and aripiprazole.
Myxedema Coma Associated with Combination Aripiprazole and Sertraline Therapy
Chelsea O Church, PharmD BCPS
Associate Professor of Pharmacy Practice, College of Pharmacy, Southwestern Oklahoma State University, Weatherford, OK
Erin C Callen, PharmD BCPS
Associate Professor of Pharmacy Practice, College of Pharmacy, Southwestern Oklahoma State University
Reprints: Dr. Church, Department of Pharmacy Practice, Southwestern Oklahoma State University College of Pharmacy, Pasteur Medical Building, Pharmacy Education, 1111 North Lee, Ste. 241, Oklahoma City, OK 73103, fax 405/601-1201, chelsea.church@swosu.edu
OBJECTIVE: To describe a case of myxedema coma (MC) associated with combination aripiprazole and sertraline therapy.
CASE SUMMARY: A 41-year-old male presented to the emergency department with confusion, right-sided numbness and tingling, slurred speech, dizziness, and facial edema. His blood pressure was 160/113 mm Hg, with a pulse of 56 beats/min and temperature of 35.4 °C. Initial abnormal laboratory values included creatine kinase (CK) 439 U/L; serum creatinine 1.6 mg/dL; aspartate aminotransferase 85 U/L; and alanine aminotransferase 35 U/L. Repeat cardiac markers revealed an elevated CK level of 3573 U/L with a CK-MB of 24 ng/mL. Thyroid function tests showed thyroid-stimulating hormone 126.4 µIU/mL and free thyroxine 0.29 ng/dL. Home medications of unknown duration were sertraline 200 mg and aripiprazole 20 mg daily. He was admitted to the intensive care unit and initially treated with intravenous levothyroxine and dexamethasone. By hospital day 4, the patient was clinically stable and discharged to home.
DISCUSSION: Myxedema coma, the most significant form of hypothyroidism (HT), is a rare but potentially fatal condition. The known precipitating causes of MC were ruled out in this patient, which left his home medications as the likely cause. Cases of HT caused by certain atypical antipsychotics and antidepressants are found in the literature, but none was reported with aripiprazole therapy. There are also no reported cases of sertraline or aripiprazole inducing MC. Use of the Naranjo probability scale indicates that the combination of aripiprazole and sertraline was a probable inducer of MC in this patient.
CONCLUSIONS: Due to the widespread use of psychotropic medications, clinicians should be reminded of the rare, yet life-threatening, occurrence of MC when treating patients, especially with combination therapies such as sertraline and aripiprazole.
Myxedema Coma Associated with Combination Aripiprazole and Sertraline Therapy
понедельник, 23 ноября 2009 г.
пятница, 20 ноября 2009 г.
среда, 18 ноября 2009 г.
mycobacterium vaccae и депрессия
Mycobacterium vaccae, a harmless bacteria normally found in dirt, has been found to stimulate the immune system of mice and boost the production of serotonin, a mood-regulating brain chemical.
The bacterium has already been successfully used in people as a vaccine against tuberculosis. It is also being tested as a treatment for cancer patients and in asthma sufferers, as a way to control the allergic reaction and help 'rebalance' the immune system.
Interest in the unusual antidepressant properties of M.vaccae arose by accident following an experimental treatment for human lung cancer led by cancer researcher Mary O'Brien at the Royal Marsden Hospital in London, England. Under that treatment, patients received heat-killed inoculations of the bacteria.
Following the tests, O'Brien's team observed not only fewer symptoms of cancer, but also improvements in their patients' vitality, emotional health and mental abilities.
Lowry and his colleagues speculated that the bacteria in these earlier experiments might have activated brain cells to release mood-lifting chemicals. To investigate the idea further, they injected heat-killed bacteria into a group of mice and found that they initiated an immune response, which activated serotonin-producing neurons in the brain.
Low levels of serotonin cause depression – an illness which afflicts around 1.3 million Australians. The most commonly prescribed antidepressant medications help treat depression by delaying the re-uptake of serotonin, thus raising levels in the brain.
According to Lowry, the strange effect of the bacteria may work by prompting the body's immune cells to release cytokines, chemicals known to activate sensory nerves that stimulate the brain. The findings are published in the journal Neuroscience.
Therapeutic Gardening against Clinical Depression
The bacterium has already been successfully used in people as a vaccine against tuberculosis. It is also being tested as a treatment for cancer patients and in asthma sufferers, as a way to control the allergic reaction and help 'rebalance' the immune system.
Interest in the unusual antidepressant properties of M.vaccae arose by accident following an experimental treatment for human lung cancer led by cancer researcher Mary O'Brien at the Royal Marsden Hospital in London, England. Under that treatment, patients received heat-killed inoculations of the bacteria.
Following the tests, O'Brien's team observed not only fewer symptoms of cancer, but also improvements in their patients' vitality, emotional health and mental abilities.
Lowry and his colleagues speculated that the bacteria in these earlier experiments might have activated brain cells to release mood-lifting chemicals. To investigate the idea further, they injected heat-killed bacteria into a group of mice and found that they initiated an immune response, which activated serotonin-producing neurons in the brain.
Low levels of serotonin cause depression – an illness which afflicts around 1.3 million Australians. The most commonly prescribed antidepressant medications help treat depression by delaying the re-uptake of serotonin, thus raising levels in the brain.
According to Lowry, the strange effect of the bacteria may work by prompting the body's immune cells to release cytokines, chemicals known to activate sensory nerves that stimulate the brain. The findings are published in the journal Neuroscience.
Therapeutic Gardening against Clinical Depression
шизофреноподобный психоз вследствие дефицита цианокобаламина
Although cobalamin deficiency is widely known and usually presents with hematologic and neuropsychiatric manifestations, the psychiatric symptoms are not usually the predominant manifestation. We describe a young single male vegetarian who developed a cobalamin-induced psychotic episode without preceding neurologic manifestations and without any hematologic symptoms. He recovered after a short course of antipsychotics and oral cobalamin supplementation and remained asymptomatic and functionally independent at 1 year of follow-up.
Schizophrenia-like psychotic episode precipitated by cobalamin deficiency.
Schizophrenia-like psychotic episode precipitated by cobalamin deficiency.
понедельник, 16 ноября 2009 г.
МРТ-предикторы шизофрении
Researchers at Columbia University led by Dr. Scott A. Small used MRI scanning to look at the brains of 18 normal adolescents, 18 youths who had schizophrenia, and 18 with preliminary symptoms. These symptoms included paranoid thinking, such as subjects believing someone was looking at them in a troubling way while knowing that’s not a realistic perception. In full schizophrenia, which affects about 1 percent of the population, people are so disconnected from reality that they believe paranoid thoughts are real.
The researchers scanned the high-risk subjects and then followed them for two years. When they looked back at the scans of those who went on to develop psychotic disorders like schizophrenia, they found 70 percent of them had shown unusually high activity in a particular part of the hippocampus, a key brain structure dealing with memory.
Is there any way to predict the onset of schizophrenia?
The researchers scanned the high-risk subjects and then followed them for two years. When they looked back at the scans of those who went on to develop psychotic disorders like schizophrenia, they found 70 percent of them had shown unusually high activity in a particular part of the hippocampus, a key brain structure dealing with memory.
Is there any way to predict the onset of schizophrenia?
четверг, 12 ноября 2009 г.
среда, 11 ноября 2009 г.
вторник, 10 ноября 2009 г.
новые алгоритмы терапии депрессии при БАР
Algorithm for the treatment of bipolar I depression
Step 1: Treat bipolar I depression for 8 weeks with
* Quetiapine 600 mg daily
or
* Lithium 0.8 mEq/L daily (or another mood stabilizer) along with lamotrigine 50 - 200 mg daily
If there is no treatment response, move on to step 2
Step 2: For treatment-resistant bipolar I depression
* Use a combination of olanzapine 6 - 12 mg plus fluoxetine 25 - 50 mg (OFC) daily
or
* Increase dose to > 600 mg of quetiapine along with lamotrigine 50 - 200 mg daily
If there is no treatment response, move on to step 3
Step 3: Treat refractory bipolar I depression
* Adjust OFC dose
or switch to
* Lithium 0.8 mEq⁄L daily plus an SSRI 20 - 40 mg and bupropion 150 - 300 mg daily
or
* Increase dose to > 600 mg of quetiapine and 20 - 40 mg of an SSRI and 150 - 300 mg of bupropion daily
or
* Use novel therapies such as modafinil or pramipexole
If there is no treatment response, move on to step 4
Step 4: Treat intractable bipolar I depression, with
* Electroconvulsive therapy
If there is still no response, the patient may have involutional bipolar I disorder
Adapted from Pacchiarotti I et al. Acta Psychiatr Scand. 2009.1
Algorithm for the treatment of bipolar II depression
Step 1: Treatment of bipolar II depression for 8 weeks with
* Lithium 0.8 mEq/L daily (or another mood stabilizer) along with lamotrigine 50 - 200 mg daily
* Quetiapine 600 mg daily
or
If there is no treatment response, move on to step 2
Step 2: For treatment-resistant bipolar I depression, use
* Lithium 0.8 mEq⁄L daily along with an SSRI 20 - 40 mg and bupropion 150 - 300 mg daily
or
* Quetiapine 300 - 600 mg daily along with an SSRI 20 - 40 mg and bupropion 150 -300 mg daily
If there is no treatment response, move on to step 3
Step 3: Treat refractory bipolar I depression
* Adjust OFC dose or switch to
* Quetiapine 300 - 600 mg daily and a monoamine oxidase inhibitor (MAOI) such as tranylcypromine 20 - 100 mg daily
or
* Lithium 0.8 mEq⁄L daily and an MAOI such as tranylcypromine 20 - 100 mg daily
or
* Novel therapies such as modafinil or pramipexole
If there is no treatment response, move on to step 4
Step 4: Treat intractable bipolar I depression with
* Electroconvulsive therapy
If there is still no response, the patient may have involutional bipolar II disorder
Adapted from Pacchiarotti I et al. Acta Psychiatr Scand. 2009.1
New Algorithms for the Management of Treatment-Resistant Bipolar Depression
Step 1: Treat bipolar I depression for 8 weeks with
* Quetiapine 600 mg daily
or
* Lithium 0.8 mEq/L daily (or another mood stabilizer) along with lamotrigine 50 - 200 mg daily
If there is no treatment response, move on to step 2
Step 2: For treatment-resistant bipolar I depression
* Use a combination of olanzapine 6 - 12 mg plus fluoxetine 25 - 50 mg (OFC) daily
or
* Increase dose to > 600 mg of quetiapine along with lamotrigine 50 - 200 mg daily
If there is no treatment response, move on to step 3
Step 3: Treat refractory bipolar I depression
* Adjust OFC dose
or switch to
* Lithium 0.8 mEq⁄L daily plus an SSRI 20 - 40 mg and bupropion 150 - 300 mg daily
or
* Increase dose to > 600 mg of quetiapine and 20 - 40 mg of an SSRI and 150 - 300 mg of bupropion daily
or
* Use novel therapies such as modafinil or pramipexole
If there is no treatment response, move on to step 4
Step 4: Treat intractable bipolar I depression, with
* Electroconvulsive therapy
If there is still no response, the patient may have involutional bipolar I disorder
Adapted from Pacchiarotti I et al. Acta Psychiatr Scand. 2009.1
Algorithm for the treatment of bipolar II depression
Step 1: Treatment of bipolar II depression for 8 weeks with
* Lithium 0.8 mEq/L daily (or another mood stabilizer) along with lamotrigine 50 - 200 mg daily
* Quetiapine 600 mg daily
or
If there is no treatment response, move on to step 2
Step 2: For treatment-resistant bipolar I depression, use
* Lithium 0.8 mEq⁄L daily along with an SSRI 20 - 40 mg and bupropion 150 - 300 mg daily
or
* Quetiapine 300 - 600 mg daily along with an SSRI 20 - 40 mg and bupropion 150 -300 mg daily
If there is no treatment response, move on to step 3
Step 3: Treat refractory bipolar I depression
* Adjust OFC dose or switch to
* Quetiapine 300 - 600 mg daily and a monoamine oxidase inhibitor (MAOI) such as tranylcypromine 20 - 100 mg daily
or
* Lithium 0.8 mEq⁄L daily and an MAOI such as tranylcypromine 20 - 100 mg daily
or
* Novel therapies such as modafinil or pramipexole
If there is no treatment response, move on to step 4
Step 4: Treat intractable bipolar I depression with
* Electroconvulsive therapy
If there is still no response, the patient may have involutional bipolar II disorder
Adapted from Pacchiarotti I et al. Acta Psychiatr Scand. 2009.1
New Algorithms for the Management of Treatment-Resistant Bipolar Depression
четверг, 5 ноября 2009 г.
Транскраниальная магнитная стимуляция в терапии резиcтентной к лечению депрессии
Of the 15 patients who participated in the study, the mean HAM-D score decreased from 29 at baseline to 11 after the treatment period. In 86% of patients, the HAM-D score decreased by at least 50%, and 57% of all patients reached remission. Three patients experienced tolerable focal pain, and this disappeared during the treatment period. No patients experienced seizure or manic symptoms.
rTMS May Be Effective in Patients With Treatment-Resistant Bipolar Depression
rTMS May Be Effective in Patients With Treatment-Resistant Bipolar Depression
вторник, 3 ноября 2009 г.
вигабатрин в терапии кокаиновой зависимости
OBJECTIVE: Cocaine dependence is associated with severe medical, psychiatric, and social morbidity, but no pharmacotherapy is approved for its treatment in the United States. The atypical antiepileptic vigabatrin ({gamma}-vinyl gamma-aminobutyric acid [GABA]) has shown promise in animal studies and open-label trials. The purpose of the present study was to assess the efficacy of vigabatrin for short-term cocaine abstinence in cocaine-dependent individuals. METHOD: Participants were treatment seeking parolees who were actively using cocaine and had a history of cocaine dependence. Subjects were randomly assigned to a fixed titration of vigabatrin (N=50) or placebo (N=53) in a 9-week double-blind trial and 4-week follow-up assessment. Cocaine use was determined by directly observed urine toxicology testing twice weekly. The primary endpoint was full abstinence for the last 3 weeks of the trial. RESULTS: Full end-of-trial abstinence was achieved in 14 vigabatrin-treated subjects (28.0%) versus four subjects in the placebo arm (7.5%). Twelve subjects in the vigabatrin group and two subjects in the placebo group maintained abstinence through the follow-up period. The retention rate was 62.0% in the vigabatrin arm versus 41.5% in the placebo arm. Among subjects who reported prestudy alcohol use, vigabatrin, relative to placebo, was associated with superior self-reported full end-of-trial abstinence from alcohol (43.5% versus 6.3%). There were no differences between the two groups in drug craving, depressed mood, anxiety, or Clinical Global Impression scores, and no group differences in adverse effects emerged. CONCLUSIONS: This first randomized, double-blind, placebo-controlled trial supports the safety and efficacy of short-term vigabatrin treatment of cocaine dependence.
Randomized, Double-Blind, Placebo-Controlled Trial of Vigabatrin for the Treatment of Cocaine Dependence in Mexican Parolees
Randomized, Double-Blind, Placebo-Controlled Trial of Vigabatrin for the Treatment of Cocaine Dependence in Mexican Parolees
понедельник, 2 ноября 2009 г.
Нелекарственная терапия при шизофрении

Treatments
Medication. All participants received Food and Drug Administration-approved antipsychotic medications for the treatment of schizophrenia, schizoaffective disorder, and schizophreniform disorder as indicated by a study psychiatrist. Medication changes were allowed, although every effort was made to stabilize participants on a tolerable and efficacious antipsychotic regimen before the initiation of psychosocial treatment. All participants were seen by a clinical nurse specialist at least biweekly to monitor medication side effects and efficacy. Most participants (>98%) were given second-generation antipsychotics throughout the study, and no significant differences emerged with regard to antipsychotic dosage, type, or clinician-estimated compliance between treatment groups. [A table detailing the between-group differences in baseline demographic, clinical, and medication characteristics is available as an online supplement to this article at ps.psychiatryonline.org.]
Cognitive enhancement therapy. CET is a comprehensive, developmental approach to the remediation of social and nonsocial cognitive deficits in schizophrenia. It seeks to facilitate the development of adult social-cognitive milestones (such as perspective taking and appraisal of one's social context) by shifting thinking from reliance on effortful, serial processing to a "gistful" and spontaneous abstraction of social themes. The treatment consists of approximately 60 hours of computer-assisted neurocognitive training in attention, memory, and problem solving and 45 social-cognitive group sessions that use experiential learning opportunities to foster the development of social wisdom and success in interpersonal interactions. A broad, theoretically driven array of social-cognitive abilities are targeted in the social-cognitive groups, which range from abstracting the "gist" or main point in social interactions to perspective taking, social context appraisal, and emotion management (39,43). Participants engage in the social-cognitive groups by responding to unrehearsed social exchanges, presenting homework, participating in cognitive exercises that focus on experiential learning, providing feedback to peers, and chairing homework sessions. CET typically begins with approximately three months of weekly one-hour neurocognitive training in attention, after which participants begin the weekly 1.5-hour social-cognitive groups. Neurocognitive training then proceeds concurrently with social-cognitive groups throughout the remaining course of treatment. A complete description of the treatment has been provided elsewhere (16).
Enriched supportive therapy. Enriched supportive therapy (EST) is an illness management and psychoeducation approach that draws on components of the basic and intermediate phases of the demonstrably effective personal therapy (44). In this approach, outpatients are seen on an individual basis to learn and practice stress management techniques designed to forestall late postdischarge relapse and enhance adjustment. The EST treatment is divided into two phases. Phase 1 focuses on basic psychoeducation about schizophrenia, the role of stress in the disorder, and ways to avoid or minimize stress. Phase 2 involves a personalized approach to the identification and management of life stressors that pose particular challenges to adequate social and role functioning. Participants move through the two phases of EST at their own pace, although each phase is typically provided for a year. By design, phase 1 was provided on a weekly basis, and phase 2 was provided on a biweekly basis. Although no attempt was made to match CET and EST approaches with regard to hours of treatment, EST served as the active control for this trial, in part to control for the potential effects on outcome of illness management and education interventions (45), which are provided in both CET and EST. All psychosocial interventions were administered by three master's-level psychiatric nurse specialists, and clinical supervision was provided by the two treatment developers.
Cognitive Enhancement Therapy for Early-Course Schizophrenia: Effects of a Two-Year Randomized Controlled Trial
понедельник, 26 октября 2009 г.
нейропсихиатрическая симптоматика СКВ в виде клиники БАР с кататоническими включениями
BACKGROUND: The American College of Rheumatology has defined 19 neuropsychiatric syndromes associated with systemic lupus erythematosus (SLE) involving the central, peripheral, and autonomic nervous systems. Neuropsychiatric manifestations of lupus (NPSLE) have been shown to occur in up to 95% of pediatric patients with SLE. OBJECTIVE: The authors describe a 15-year-old African American young woman with a family history positive for bipolar I disorder and schizophrenia, who presented with symptoms consistent with an affective disorder. METHOD: The patient was diagnosed with Bipolar I disorder with catatonic features and required multiple hospitalizations for mood disturbance. Two years after her initial presentation, the patient was noted to have a malar rash and subsequently underwent a full rheumatologic work-up, which revealed cerebral vasculitis. RESULTS: NPSLE was diagnosed and, after treatment with steroids, the patient improved substantially and no longer required further psychiatric medication or therapy. CONCLUSION: Given the especially high prevalence of NPSLE in pediatric patients with lupus, it is important for clinicians to recognize that neuropsychiatric symptoms in an adolescent patient may indeed be the initial manifestations of SLE, as opposed to a primary affective disorder.
Neuropsychiatric Systemic Lupus Erythematosus Presenting as Bipolar I Disorder With Catatonic Features
Neuropsychiatric Systemic Lupus Erythematosus Presenting as Bipolar I Disorder With Catatonic Features
четверг, 22 октября 2009 г.
повышенное количество маркеров воспаления при шизофрении и бар
Sigrun Hope, from the University of Oslo, and colleagues therefore measured plasma soluble tumor necrosis factor receptor 1 (sTNF-R1), interleukin (IL)-1 receptor antagonist (IL-1Ra), IL-6, high-sensitivity C reactive protein (hs-CRP), soluble CD40L ligand (sCD40L), and von Willebrand factor (vWF) levels in 125 bipolar disorder patients, 186 schizophrenia patients, and 244 healthy controls.
The findings, published in the journal Bipolar Disorders, indicate the combined patient groups had significantly higher plasma levels of sTNF-R1 and vWF compared with healthy controls, at increases of 17% and 27%, respectively. While hs-CRP levels were significantly increased in patients versus controls, at an average of 0.95 ng/ml versus 0.80 ng/ml, there were no significant differences for the other inflammatory markers.
The team also found that unmedicated bipolar disorder and schizophrenia patients had significantly increased levels of sTNF-R1 and vWF compared with controls, at1.09 versus 0.91 ng/ml and 101 versus 77%, respectively. There were no significant differences between bipolar disorder and schizophrenia patients, regardless of medication status.
The findings were unaffected by controlling for age, gender, ethnicity, liver function, kidney function, cardiovascular disorder, diabetes, and alcohol intake, as well as for hs-CRP levels.
Inflammatory markers increased in bipolar disorder and schizophrenia
The findings, published in the journal Bipolar Disorders, indicate the combined patient groups had significantly higher plasma levels of sTNF-R1 and vWF compared with healthy controls, at increases of 17% and 27%, respectively. While hs-CRP levels were significantly increased in patients versus controls, at an average of 0.95 ng/ml versus 0.80 ng/ml, there were no significant differences for the other inflammatory markers.
The team also found that unmedicated bipolar disorder and schizophrenia patients had significantly increased levels of sTNF-R1 and vWF compared with controls, at1.09 versus 0.91 ng/ml and 101 versus 77%, respectively. There were no significant differences between bipolar disorder and schizophrenia patients, regardless of medication status.
The findings were unaffected by controlling for age, gender, ethnicity, liver function, kidney function, cardiovascular disorder, diabetes, and alcohol intake, as well as for hs-CRP levels.
Inflammatory markers increased in bipolar disorder and schizophrenia
понедельник, 19 октября 2009 г.
Средиземноморская диета снижает риск возникновения депрессии
Dr. Martinez-Gonzalez said the risk for depression was substantially lower in participants with higher adherence to the MDP and that depression rates were about 30% lower in those with the highest consumption of fruit, nuts, legumes, and monounsaturated vs saturated fats.
"The important thing regarding fish is that a very low consumption of fish (lowest quintile) was in fact a risk factor when it was compared with the 3 upper categories of fish consumption (merged together)," he added.
The researchers were trying to determine why the lifetime prevalence of mental disorders is lower in Mediterranean than Northern European countries. One possible factor is diet, as previous research has suggested that the monounsaturated fatty acids in olive oil — used abundantly in the Mediterranean diet — may be associated with a lower risk for severe depressive symptoms.
The study included 10,094 healthy Spanish participants who reported their dietary intake on a food frequency questionnaire. After a median follow-up of 4.4 years, there were 480 new cases of depression. Individuals who followed the Mediterranean diet most closely had a greater than 30% reduction in the risk for depression than whose who had the lowest Mediterranean diet scores. The association did not change when the results were adjusted for other markers of a healthy lifestyle.
The strength of the inverse association between the [MDP] and depression surprised the investigators. "The new question for us is that if these results will be reproduced in a primary prevention trial," Dr. Martinez-Gonzalez said. "Another new question is whether the MDP is longitudinally associated with increased serum levels of BDNF," or brain-derived neurotrophic factor — a peptide critical for axonal growth, neuronal survival, and synaptic plasticity.
According to the authors, "An emerging concept in neuroscience is that perturbations in the health of cerebral endothelium (such as some loss of the neuroprotection afforded by BDNF) may mediate progressive neuronal dysfunction." Depression is associated with low BDNF in some patients.
Mediterranean Diet Cut Depression Risk by 30%
"The important thing regarding fish is that a very low consumption of fish (lowest quintile) was in fact a risk factor when it was compared with the 3 upper categories of fish consumption (merged together)," he added.
The researchers were trying to determine why the lifetime prevalence of mental disorders is lower in Mediterranean than Northern European countries. One possible factor is diet, as previous research has suggested that the monounsaturated fatty acids in olive oil — used abundantly in the Mediterranean diet — may be associated with a lower risk for severe depressive symptoms.
The study included 10,094 healthy Spanish participants who reported their dietary intake on a food frequency questionnaire. After a median follow-up of 4.4 years, there were 480 new cases of depression. Individuals who followed the Mediterranean diet most closely had a greater than 30% reduction in the risk for depression than whose who had the lowest Mediterranean diet scores. The association did not change when the results were adjusted for other markers of a healthy lifestyle.
The strength of the inverse association between the [MDP] and depression surprised the investigators. "The new question for us is that if these results will be reproduced in a primary prevention trial," Dr. Martinez-Gonzalez said. "Another new question is whether the MDP is longitudinally associated with increased serum levels of BDNF," or brain-derived neurotrophic factor — a peptide critical for axonal growth, neuronal survival, and synaptic plasticity.
According to the authors, "An emerging concept in neuroscience is that perturbations in the health of cerebral endothelium (such as some loss of the neuroprotection afforded by BDNF) may mediate progressive neuronal dysfunction." Depression is associated with low BDNF in some patients.
Mediterranean Diet Cut Depression Risk by 30%
пятница, 16 октября 2009 г.
депрессия и фолиевая кислота
Instead, the men were referring to medical foods - more specifically, a new product called Deplin, a medical food that includes L-methylfolate, the only active form of folate that can cross the blood brain barrier and help with the synthesis of the neurotransmitters associated with mood and, consequently, mood disorders such as depression: serotonin, dopamine, and norepinephrine.
Research shows that people with depression and low folate levels are less likely to respond to treatments such as antidepressants and less likely to achieve remission.
Treating Depression and Folate Deficiency With Medical Foods
Research shows that people with depression and low folate levels are less likely to respond to treatments such as antidepressants and less likely to achieve remission.
Treating Depression and Folate Deficiency With Medical Foods
отравление бергамотом
A 44-year-old man presented in May, 2001, with muscle cramps. He had no medical history of note, but volunteered the fact that he had been drinking up to 4 L of black tea per day over the past 25 years. His preferred brand was GoldTeefix (Tekanne, Salzburg, Austria). Since this type of tea had given him occasional gastric pain, he changed to Earl Grey (Twinings & Company, London, UK), which he thought would be less harmful to his stomach. 1 week after the change, he noticed repeated muscle cramps for some seconds in his right foot. The longer he drank Earl Grey tea, the more intense the muscle cramps became. After 3 weeks, they also occurred in the left foot...
Earl Grey tea is composed of black tea and the essence of bergamot oil, an extract from the rind of bergamot orange (Citrus aurantium ssp bergamia), which has a pleasant, refreshing scent. Bergamot oil contains bergapten (5-methoxypsoralen), bergamottin (5-geranyloxypsoralen), and citropten (5,7-dimethoxycoumarin), which can be found in grapefruit juice, celery, parsnips, and Seville orange juice. Bergamot oil is a well-known UVA-induced photosensitiser with a strong phototoxic effect, and is used therapeutically in psoriasis, vitiligo, mycosis fungoides, and cutaneous lymphoma. Because of this side-effect, bergamot oil has been widely banned as an ingredient in cosmetics and tanning products. Bergamot oil also has a hepatotoxic effect and may cause contact-allergy. The adverse effects of bergamot oil in this patient are explained by the effect of bergapten as a largely selective axolemmal potassium channel blocker, reducing potassium permeability at the nodes of Ranvier in a time-dependent manner. This may lead to hyperexcitability of the axonal membrane and phasic alterations of potassium currents, causing fasciculations and muscle cramps.
Tea intoxication
Earl Grey tea is composed of black tea and the essence of bergamot oil, an extract from the rind of bergamot orange (Citrus aurantium ssp bergamia), which has a pleasant, refreshing scent. Bergamot oil contains bergapten (5-methoxypsoralen), bergamottin (5-geranyloxypsoralen), and citropten (5,7-dimethoxycoumarin), which can be found in grapefruit juice, celery, parsnips, and Seville orange juice. Bergamot oil is a well-known UVA-induced photosensitiser with a strong phototoxic effect, and is used therapeutically in psoriasis, vitiligo, mycosis fungoides, and cutaneous lymphoma. Because of this side-effect, bergamot oil has been widely banned as an ingredient in cosmetics and tanning products. Bergamot oil also has a hepatotoxic effect and may cause contact-allergy. The adverse effects of bergamot oil in this patient are explained by the effect of bergapten as a largely selective axolemmal potassium channel blocker, reducing potassium permeability at the nodes of Ranvier in a time-dependent manner. This may lead to hyperexcitability of the axonal membrane and phasic alterations of potassium currents, causing fasciculations and muscle cramps.
Tea intoxication
среда, 14 октября 2009 г.
вторник, 13 октября 2009 г.

Илоперидон
QT Prolongation: In an open-label QTc study in patients with schizophrenia or schizoaffective disorder (N=160), Fanapt was associated with QTc prolongation of 9 msec at an iloperidone dose of 12 mg twice daily. This affect was augmented by the presence of CYP450, 2D6 or 3A4 metabolic inhibition. The use of Fanapt should be avoided in combination with other drugs that are known to prolong QTc. Caution is warranted when prescribing Fanapt with drugs that inhibit Fanapt metabolism.
Weight Gain: Based on the pooled data from the four placebo-controlled, 4- or 6-week, fixed- or flexible-dose studies, the proportions of patients having a weight gain of greater than or equal to 7% body weight was 12% for Fanapt 10-16 mg/day, 18% for Fanapt 20-24 mg/day, and 13% for Fanapt (combined doses) versus 4% for placebo.
Orthostatic Hypotension and Syncope: Fanapt can induce orthostatic hypotension and syncope. Fanapt should be used with caution in patients with known cardiovascular disease, cerebrovascular disease, or conditions that predispose the patient to hypotension.
Leukopenia, Neutropenia, and Agranulocytosis: In clinical trial and postmarketing experience, events of leukopenia/neutropenia have been reported temporally related to antipsychotic agents. Agranulocytosis (including fatal cases) have been reported. Patients with a pre-existing low white blood cell count (WBC) or a history of leukopenia/neutropenia should have their complete blood count (CBC) monitored frequently during the first few months of therapy and should discontinue Fanapt at the first sign of a decline in WBC in the absence of other causative factors.
Hyperprolactinemia: As with other drugs that antagonize dopamine D2 receptors, Fanapt elevates prolactin levels. Galactorrhea, amenorrhea, gynecomastia and impotence have been reported in patients receiving prolactin-elevating compounds.
Novartis Enters Into Agreement for Exclusive US and Canadian Rights to Fanapt(TM), an FDA-Approved Oral Therapy for Schizophrenia
Weight Gain: Based on the pooled data from the four placebo-controlled, 4- or 6-week, fixed- or flexible-dose studies, the proportions of patients having a weight gain of greater than or equal to 7% body weight was 12% for Fanapt 10-16 mg/day, 18% for Fanapt 20-24 mg/day, and 13% for Fanapt (combined doses) versus 4% for placebo.
Orthostatic Hypotension and Syncope: Fanapt can induce orthostatic hypotension and syncope. Fanapt should be used with caution in patients with known cardiovascular disease, cerebrovascular disease, or conditions that predispose the patient to hypotension.
Leukopenia, Neutropenia, and Agranulocytosis: In clinical trial and postmarketing experience, events of leukopenia/neutropenia have been reported temporally related to antipsychotic agents. Agranulocytosis (including fatal cases) have been reported. Patients with a pre-existing low white blood cell count (WBC) or a history of leukopenia/neutropenia should have their complete blood count (CBC) monitored frequently during the first few months of therapy and should discontinue Fanapt at the first sign of a decline in WBC in the absence of other causative factors.
Hyperprolactinemia: As with other drugs that antagonize dopamine D2 receptors, Fanapt elevates prolactin levels. Galactorrhea, amenorrhea, gynecomastia and impotence have been reported in patients receiving prolactin-elevating compounds.
Novartis Enters Into Agreement for Exclusive US and Canadian Rights to Fanapt(TM), an FDA-Approved Oral Therapy for Schizophrenia
понедельник, 12 октября 2009 г.
Кортизол и память
В Лейденском университете защищена диссертация на тему ''Ускользающее из памяти'' (ориг. на англ. ''Fading memories''). Автор работы - M.Tollenaar (ф-т социальных наук). Исследование посвящено непосредственным и долговременным эффектам гормонов стресса на способность вспомнить что-либо. Исследовательница изучала прежде всего гормоны стресс: кортизол и (нор)адреналин. Диссертация показывает, что стресс или добавление кортизола приводят к ухудшению памяти. Эти эффекты лучше всего просматривались при попытке воспроизведения заученных слов, но практически не затрагивали личные воспоминания. Если под воздействием только стресса люди затруднялись припомнить менее эмоциональные слова, то при добавлении кортизола они уже хуже справлялись с задачей припоминания нейтральных слов. Самым важной новой находкой является то, что острый стресс в сочетании с некоторой дозой кортизола производит также долговременный эффект в части воспоминания нейтральных и эмоциональных слов. Автор не обнаружила воздействия стресса и кортизола на эмоциональные переживания воспоминаний. Исследовательница планирует в будущем исследовать эффекты гормонов стресса на автобиографические воспоминания. Это позволит лучше понять применение кортизола и пропранолола в клинической практике.
МНИИП
МНИИП
воскресенье, 11 октября 2009 г.
Нейролептики при деменции
После рекомендации воздерживаться от употребления атипичных нейролептиков из-за повышенного риска инсультов, Trifiro отметил убедительный рост количества назначений классических антипсихотиков. Но эти препараты несут такой же высокий (зависимый от дозы) риск инсульта, что и атипичные антипсихотики, по сравнению с пациентами, которые не принимали никаких психотропных препаратов. В некоторых подгруппах классических нейролептиков риск намного выше, в частности, 5,8 для фенотиазинов и 3,6 для бутирофенонов (например, галоперидола). Trifiro призывает максимально ограничить использование обоих классов лекарств. ''Употреблять их только при необходимости, в самых низких дозах и в течение максимально короткого времени''. Trifiro не отмечает при использовании классических антипсихотиков повышенного риска (в т.ч. фатальной) пневмонии, по сравнению с атипичными антипсихотиками. Вместе с тем, он ожидал повышенных рисков в связи с действием на экстрапирамидную систему, что вызывает акинезию и впоследствии может вызвать аспирационную пневмонию. Но, как оказалось, летальные случаи от воспаления легких чаще встречались при использовании атипичных антипсихотиков. Вероятность пневмонии возрастает в связи с аффинитетом антипсихотиков к гистаминергическим рецепторам Н1. Именно поэтому у фенотиазинов самый высокий сравнительный риск 4,3 – по сравнению с пациентами, которые не принимают психотропных препаратов. Trifiro объясняет это тем, что гистаминовые рецепторы участвую в седации, а седация может создавать проблемы с глотанием и впоследствии аспирационную пневмонию.
МНИИП
МНИИП
вторник, 29 сентября 2009 г.
из Iloperidone for schizophrenia
Pharmacokinetics
Iloperidone is administered twice daily and can be taken with or without food. The bioavailability of iloperidone tablets is 96%, and peak plasma concentrations are achieved 2 to 4 hours after ingestion.
Like all antipsychotics except paliperidone, iloperidone is metabolized by the liver’s cytochrome P450 (CYP) system. The enzyme pathways CYP3A4 and CYP2D6 transform iloperidone into 2 metabolites: one with CNS activity (P88) and one that does not cross the blood-brain barrier and is not active in the CNS (P95) but likely has peripheral effects.
Genetic variations in CYP2D6 activity can substantially alter how individual patients metabolize iloperidone. The half-life of iloperidone and its active metabolites differs depending on whether someone is a poor metabolizer (no functional CYP2D6 activity), intermediate metabolizer (reduced CYP2D6 activity), or extensive metabolizer (“normal” CYP2D6 activity). The usual half-life of iloperidone (approximately 18 hours in extensive metabolizers) can be almost 50% longer (>24 hours) in CYP2D6 poor metabolizers.
There are no recommendations to test patients for genetic variants that result in poor metabolism from CYP2D6. Rather, clinicians simply need to be aware that this could be the source of interindividual differences they see in iloperidone tolerability, just as it is for any other medication that is a substrate for the CYP2D6 enzyme system.
Interactions. Medications that inhibit the CYP3A4 or CYP2D6 systems can increase iloperidone plasma level when taken concurrently with iloperidone, even if intrinsic liver metabolism activity is normal. Fluoxetine and paroxetine are potent CYP2D6 inhibitors. Concurrent treatment with either of these selective serotonin reuptake inhibitors could increase iloperidone plasma concentration by 100% or more.4
Similarly, cotreatment with a potent CYP3A4 inhibitor such as ketoconazole (or drinking grapefruit juice) will decrease metabolism and increase plasma concentrations of iloperidone and its active metabolites by about 50%. Smoking status should not influence iloperidone plasma concentration because this drug is not a primary substrate for CYP1A2, the enzyme induced by cigarette smoking.
The bottom line: reduce iloperidone dosage by 50% for patients who are taking a strong CYP2D6 and/or CYP3A4 inhibitor (see Dosing below).
Relative receptor binding affinities of 3 atypical antipsychotics*понедельник, 28 сентября 2009 г.
Врач-иммунолог Roos Padmos посвятила свою диссертацию исследованию связи между биполярными расстройствами и аутоиммунными заболеваниями, и исследовала определенную клетку иммунной системы (моноциты) на предмет отклонений в экспрессии генов. Она обнаружила возможный ключевой ген – PDE4B, который играет главную роль не только в иммунной системе, но и при расстройствах настроения.
Drexhage: ''Есть препарат против PDE4 – Rolipram. Он раньше применялся как антидепрессант. Он вызывал сильную тошноту, и его перестали выписывать. Сейчас разработаны новые версии этого препарата, которые используются как противовоспалительное средство. Я бы хотел исследовать его как новый антидепрессант. В целом, все антипсихотики и антидепрессанты производят антивоспалительный эффект''.
...
'Интерферон-альфа – антивирусный препарат, который назначают при гепатите С. Я сотрудничаю с коллегой из Лондона, который использует этот препарат, и вот что оказалось: у 60% его пациентов после трех месяцев еженедельного приема препарата обнаружились признаки тяжелой депрессии.
''Эти 60% обладают определенными интерлейкиновыми рецепторами (цитокинные рецепторы, играющие роль в системе защиты организма), которые делают человека уязвимым для депрессии. У оставшихся 40% - другой тип рецепторов, и у них никогда не будет депрессии от приема интерферона-альфа.
...
''Цитокины TNF, которые играют роль при аутоиммунных заболеваниях, можно притормозить с помощью препарата Etanercept (анти-TNF), используемого в лечении псориаза. И – что интересно – он больше воздействует на депрессию при псориазе, и меньше на сам псориаз...
С заболеваниями щитовидной железы – к психиатру
Drexhage: ''Есть препарат против PDE4 – Rolipram. Он раньше применялся как антидепрессант. Он вызывал сильную тошноту, и его перестали выписывать. Сейчас разработаны новые версии этого препарата, которые используются как противовоспалительное средство. Я бы хотел исследовать его как новый антидепрессант. В целом, все антипсихотики и антидепрессанты производят антивоспалительный эффект''.
...
'Интерферон-альфа – антивирусный препарат, который назначают при гепатите С. Я сотрудничаю с коллегой из Лондона, который использует этот препарат, и вот что оказалось: у 60% его пациентов после трех месяцев еженедельного приема препарата обнаружились признаки тяжелой депрессии.
''Эти 60% обладают определенными интерлейкиновыми рецепторами (цитокинные рецепторы, играющие роль в системе защиты организма), которые делают человека уязвимым для депрессии. У оставшихся 40% - другой тип рецепторов, и у них никогда не будет депрессии от приема интерферона-альфа.
...
''Цитокины TNF, которые играют роль при аутоиммунных заболеваниях, можно притормозить с помощью препарата Etanercept (анти-TNF), используемого в лечении псориаза. И – что интересно – он больше воздействует на депрессию при псориазе, и меньше на сам псориаз...
С заболеваниями щитовидной железы – к психиатру
вторник, 22 сентября 2009 г.
пятница, 18 сентября 2009 г.
Пестициды - одни из главных виновников развития болезни Паркинсона
Люди, которые подвергаются воздействию пестицидов, имеют повышенный риск развития болезни Паркинсона. Медики подозревают, что пестициды из-за своего едкого химического состава являются одними из главных виновников развития дегенеративного расстройства, поэтому в группе особого риска проблем со здоровьем находятся работники сельского хозяйства.
Врачи Института Паркинсона /Калифорния, США/ рассмотрели здоровье 519 пациентов с диагностированным условием и 511 здоровых человек из контрольной группы одинакового возраста и проживающих в одном и том же географическом регионе. Особое внимание учёные обратили на воздействие токсинов на здоровье участников, в том числе пестицидов и растворителей.
Среди пациентов с болезнью Паркинсона 8,5% подвергались сильному воздействию химикатов. В двух группах профессиональное влияние пестицидов на здоровье ассоциировалось с высоким риском заболевания. Специалисты определили восемь пестицидов, которые обладали самыми активными нейротоксическими свойствами и в два раза увеличивали вероятность паркинсонизма.
Три химиката троекратно повышали риск болезни Паркинсона: хлорорганические соединения, средства от сорняков /гербициды/ и инсектициды против насекомых. Все идентифицированные составы повреждали работу нейронов в мозге и способствовали умственной дисфункции. Неврологи намерены в дальнейшем оценить опасность применения пестицидов в садоводстве и употребления в пищу фруктов и овощей, обработанных химикатами.
http://www.medlinks.ru/article.php?sid=37884
Врачи Института Паркинсона /Калифорния, США/ рассмотрели здоровье 519 пациентов с диагностированным условием и 511 здоровых человек из контрольной группы одинакового возраста и проживающих в одном и том же географическом регионе. Особое внимание учёные обратили на воздействие токсинов на здоровье участников, в том числе пестицидов и растворителей.
Среди пациентов с болезнью Паркинсона 8,5% подвергались сильному воздействию химикатов. В двух группах профессиональное влияние пестицидов на здоровье ассоциировалось с высоким риском заболевания. Специалисты определили восемь пестицидов, которые обладали самыми активными нейротоксическими свойствами и в два раза увеличивали вероятность паркинсонизма.
Три химиката троекратно повышали риск болезни Паркинсона: хлорорганические соединения, средства от сорняков /гербициды/ и инсектициды против насекомых. Все идентифицированные составы повреждали работу нейронов в мозге и способствовали умственной дисфункции. Неврологи намерены в дальнейшем оценить опасность применения пестицидов в садоводстве и употребления в пищу фруктов и овощей, обработанных химикатами.
http://www.medlinks.ru/article.php?sid=37884
Детская деменция
Isobel was diagnosed with early on set dementia, aged just nine, when she began to slur her words and display the same problems as people eight times her age.
Child dementia affects around one in twelve million youngsters around the world, but is sometimes treatable.
There are 100 different types of dementia, including Alzheimer's, but doctors say Isobel's condition is unique and she has not responded to any medication.
Schoolgirl diagnosed with dementia
Child dementia affects around one in twelve million youngsters around the world, but is sometimes treatable.
There are 100 different types of dementia, including Alzheimer's, but doctors say Isobel's condition is unique and she has not responded to any medication.
Schoolgirl diagnosed with dementia
вторник, 15 сентября 2009 г.
понедельник, 14 сентября 2009 г.
предикторы эффективности антидепрессантов
A new medical test — called a biomarker test — appears to help predict a patient’s response to a specific antidepressant. The test is non-invasive, painless and fast, taking about 15 minutes. Six electrodes (which measure brain activity) are placed around the forehead and on the earlobes (the electrodes don’t hurt — they are only measuring devices).
Here’s what the study found:
Subjects were then randomly assigned to continue with escitalopram or were given a different drug. A total of 73 patients who remained on escitalopram were tracked for 49 days to see if their results matched the prediction of the ATR biomarker. The ATR predicted both response and remission with an accuracy rate of 74 percent, much higher than any other method available.
The researchers also found that they could predict whether subjects were more likely to respond to a different antidepressant, bupropion, also known as Wellbutrin XL.
Test Predicts Depression Medication Response
Here’s what the study found:
Subjects were then randomly assigned to continue with escitalopram or were given a different drug. A total of 73 patients who remained on escitalopram were tracked for 49 days to see if their results matched the prediction of the ATR biomarker. The ATR predicted both response and remission with an accuracy rate of 74 percent, much higher than any other method available.
The researchers also found that they could predict whether subjects were more likely to respond to a different antidepressant, bupropion, also known as Wellbutrin XL.
Test Predicts Depression Medication Response
пятница, 11 сентября 2009 г.
Кетамин быстро и эффективно устраняет суицидальные наклонности у больных депрессией
Небольшое исследование американских ученых показало, что препарат для внутривенного наркоза кетамин, который является также сильным диссоциативным галлюциногеном, быстро и эффективно устраняет суицидальные наклонности у больных депрессией, сообщает EurekAlert!.
В психиатрической практике нередко встречаются ситуации, когда депрессивного больного преследуют мысли о самоубийстве. Поскольку существующие антидепрессанты начинают действовать лишь через несколько недель после начала лечения, их использование в подобных ситуациях малоэффективно – пациент может свести счеты с жизнью, не дождавшись эффекта от терапии.
Исследователи из Медицинской школы Маунт Синай в Нью-Йорке назначили небольшой группе пациентов с депрессией, склонных к самоубийству, экспериментальное лечение внутривенными инъекциями кетамина.
Выяснилось, что однократное введение этого препарата резко и значительно подавляло суицидальные мысли у пациентов на протяжении по меньшей мере суток после инъекции. Этот эффект существенно продлевался при введении повторных доз кетамина в течение двух недель.
По мнению одной из исследователей Ребекки Прайс (Rebecca Price), если результаты работы подтвердятся в более масштабных испытаниях, внутривенное введение кетамина может стать предпочтительным лечением в тех случаях, когда ожидание эффекта традиционных антидепрессантов ставит под угрозу жизнь пациентов.
http://www.medlinks.ru/article.php?sid=37775
В психиатрической практике нередко встречаются ситуации, когда депрессивного больного преследуют мысли о самоубийстве. Поскольку существующие антидепрессанты начинают действовать лишь через несколько недель после начала лечения, их использование в подобных ситуациях малоэффективно – пациент может свести счеты с жизнью, не дождавшись эффекта от терапии.
Исследователи из Медицинской школы Маунт Синай в Нью-Йорке назначили небольшой группе пациентов с депрессией, склонных к самоубийству, экспериментальное лечение внутривенными инъекциями кетамина.
Выяснилось, что однократное введение этого препарата резко и значительно подавляло суицидальные мысли у пациентов на протяжении по меньшей мере суток после инъекции. Этот эффект существенно продлевался при введении повторных доз кетамина в течение двух недель.
По мнению одной из исследователей Ребекки Прайс (Rebecca Price), если результаты работы подтвердятся в более масштабных испытаниях, внутривенное введение кетамина может стать предпочтительным лечением в тех случаях, когда ожидание эффекта традиционных антидепрессантов ставит под угрозу жизнь пациентов.
http://www.medlinks.ru/article.php?sid=37775
понедельник, 7 сентября 2009 г.
Азенапин
A new antipsychotic drug, asenapine, has been approved by the Food and Drug Administration (FDA) for the acute treatment of schizophrenia and manic or mixed episode in bipolar I disorder in adults.
Similar to other second-generation antipsychotics, asenapine is an antagonist of the serotonin 5HT2 and dopamine D2 receptors.
In the long-term schizophrenia trial, three of the 908 patients (0.3 percent) treated with asenapine had a QTc interval increase from baseline of greater than 60 msec. None had a QTc interval increase of 500 msec or more.
Asenapine is formulated as sublingual tablets to optimize its bioavailability upon absorption, since the drug is extensively metabolized in the liver. The tablet should not be swallowed. The approved dosage for acute schizophrenia treatment is 5 mg twice daily. The dosage for bipolar I disorder is to start with 10 mg twice daily with the option of decreasing to 5 mg twice daily if the patient experiences adverse effects.
Asenapine Adds to Arsenal to Treat Psychotic Disorders
Similar to other second-generation antipsychotics, asenapine is an antagonist of the serotonin 5HT2 and dopamine D2 receptors.
In the long-term schizophrenia trial, three of the 908 patients (0.3 percent) treated with asenapine had a QTc interval increase from baseline of greater than 60 msec. None had a QTc interval increase of 500 msec or more.
Asenapine is formulated as sublingual tablets to optimize its bioavailability upon absorption, since the drug is extensively metabolized in the liver. The tablet should not be swallowed. The approved dosage for acute schizophrenia treatment is 5 mg twice daily. The dosage for bipolar I disorder is to start with 10 mg twice daily with the option of decreasing to 5 mg twice daily if the patient experiences adverse effects.
Asenapine Adds to Arsenal to Treat Psychotic Disorders
среда, 2 сентября 2009 г.
психоз индуцированный терапией радиоактивным йодом
Because of enlarged lymph nodes and suspected residual cancer cells, she received radioactive iodine treatment in May 2008. The next day she developed paranoid delusions that her home was bugged by various electrical devices. She thought her conversations were being recorded, and she insisted that her husband leave his cell phone and other electronic devices in his car. She developed ideas of reference that the headlines in magazines and newspapers were sending her personal messages. The patient had no prior psychiatric history and did not receive a psychiatric evaluation until November 2008, at which time she also had laboratory and imaging studies. Her thyroid-stimulating hormone level, free T4 level, electrolytes, complete blood count, toxicology screen, and brain magnetic resonance imaging were all normal. and brain magnetic resonance imaging were all normal.
At this point, Ms. T was given a diagnosis of radioactive iodine-induced psychotic disorder and was treated with risperidone, 0.5 mg at bedtime. At a follow-up appointment 1 week later, she reported being almost free of any paranoid thoughts or ideas of reference.
Radioactive Iodine-Induced Psychosis
At this point, Ms. T was given a diagnosis of radioactive iodine-induced psychotic disorder and was treated with risperidone, 0.5 mg at bedtime. At a follow-up appointment 1 week later, she reported being almost free of any paranoid thoughts or ideas of reference.
Radioactive Iodine-Induced Psychosis
вторник, 1 сентября 2009 г.


понедельник, 31 августа 2009 г.
Lurasidone Demonstrated Efficacy In Treating Patients - phase 3 study
Lurasidone 40 and 120 mg, taken once-daily, demonstrated significantly greater improvement versus placebo on the primary efficacy measure, the Positive and Negative Syndrome Scale (PANSS) total score, at study endpoint. PANSS score changes from baseline for lurasidone 40 and 120 mg/day versus placebo were -25.7 and -23.6 vs. -16.0, respectively, at study endpoint. A total of 53% of patients on lurasidone 40 mg/day and 47% of patients on lurasidone 120 mg/day demonstrated a 30% or more improvement on the PANSS total score from baseline versus 38% on placebo.
The effect of lurasidone on weight was similar to placebo, median weight change: 0.9 kg (2 lbs) for 40 mg/day, 0.5 kg (1.1lbs) for 120 mg/day vs. 0 kg for placebo at study endpoint. The incidence of clinically significant weight gain (greater than or equal to 7% increase from baseline to study endpoint) was 7.6% for lurasidone 40 mg/day, 4.2% for lurasidone 120 mg/day and 7.0% for placebo.
Lurasidone was also well-tolerated with an overall discontinuation rate similar to placebo (40% vs. 39% placebo) and few adverse event-related discontinuations (9% for both the overall lurasidone group and placebo). Adverse events seen in the trial were generally mild. The most commonly reported adverse events for lurasidone 40 and 120 mg/day combined (greater than 5% and at least twice the rate of placebo) were akathisia (17.3% vs. 0.9% placebo), somnolence (12.2% vs. 4.3% placebo), sedation (11.4% vs. 3.4% placebo), parkinsonism (10.1% vs. 1.7% placebo), nausea (9.3% vs. 4.3% placebo), and dystonia (5.5% vs. 0.9% placebo).
Lurasidone is an atypical antipsychotic discovered and developed by DSP with a unique chemical structure. Lurasidone has high affinities for dopamine D2, serotonin 5-HT7, 5-HT2A, 5-HT1A, and noradrenalin alpha2C receptors and minimal-to-no affinity for histamine H1 or cholinergic M1 receptors.
Thread: Lurasidone Demonstrated Efficacy In Treating Patients - phase 3 study
The effect of lurasidone on weight was similar to placebo, median weight change: 0.9 kg (2 lbs) for 40 mg/day, 0.5 kg (1.1lbs) for 120 mg/day vs. 0 kg for placebo at study endpoint. The incidence of clinically significant weight gain (greater than or equal to 7% increase from baseline to study endpoint) was 7.6% for lurasidone 40 mg/day, 4.2% for lurasidone 120 mg/day and 7.0% for placebo.
Lurasidone was also well-tolerated with an overall discontinuation rate similar to placebo (40% vs. 39% placebo) and few adverse event-related discontinuations (9% for both the overall lurasidone group and placebo). Adverse events seen in the trial were generally mild. The most commonly reported adverse events for lurasidone 40 and 120 mg/day combined (greater than 5% and at least twice the rate of placebo) were akathisia (17.3% vs. 0.9% placebo), somnolence (12.2% vs. 4.3% placebo), sedation (11.4% vs. 3.4% placebo), parkinsonism (10.1% vs. 1.7% placebo), nausea (9.3% vs. 4.3% placebo), and dystonia (5.5% vs. 0.9% placebo).
Lurasidone is an atypical antipsychotic discovered and developed by DSP with a unique chemical structure. Lurasidone has high affinities for dopamine D2, serotonin 5-HT7, 5-HT2A, 5-HT1A, and noradrenalin alpha2C receptors and minimal-to-no affinity for histamine H1 or cholinergic M1 receptors.
Thread: Lurasidone Demonstrated Efficacy In Treating Patients - phase 3 study
Комбинация сертралина с оланзапином в терапии психотической депрессии
At the conclusion of the 12-week trial, investigators found that treatment with olanzapine/sertraline was associated with higher remission rates during the trial than olanzapine/placebo (odds ratio, 1.28; 95% confidence interval, 1.12 – 1.47; P < .001) and that 49% of subjects in the combination therapy group were in remission at their last assessment vs 23.9% of those treated with olanzapine alone.
In addition, the study showed that combination therapy was comparably superior in both younger and older age groups. Although both age groups experienced significant increases in cholesterol and triglyceride concentrations, statistically significant increases in glucose occurred in younger adults.
Further, whereas both age groups experienced weight gain, younger adults gained significantly more weight than their older counterparts — a mean gain of 6.5 vs 3.3 kg.
The study findings suggest that combination therapy is effective and offers physicians and their patients a viable alternative to electroconvulsive therapy, which is generally considered the treatment of choice for this condition but is not without challenges.
The researchers note that although bilateral electroconvulsive therapy has a response rate of 87% when administered in academic centers, the response when delivered in the community setting is much lower, ranging from 30% to 47%. Further, they add, pharmacological treatment may be more practical and less stigmatizing for patients.
STOP-PD: Combination Therapy With Sertraline Plus Olanzapine Effective in the Treatment of Psychotic Depression
In addition, the study showed that combination therapy was comparably superior in both younger and older age groups. Although both age groups experienced significant increases in cholesterol and triglyceride concentrations, statistically significant increases in glucose occurred in younger adults.
Further, whereas both age groups experienced weight gain, younger adults gained significantly more weight than their older counterparts — a mean gain of 6.5 vs 3.3 kg.
The study findings suggest that combination therapy is effective and offers physicians and their patients a viable alternative to electroconvulsive therapy, which is generally considered the treatment of choice for this condition but is not without challenges.
The researchers note that although bilateral electroconvulsive therapy has a response rate of 87% when administered in academic centers, the response when delivered in the community setting is much lower, ranging from 30% to 47%. Further, they add, pharmacological treatment may be more practical and less stigmatizing for patients.
STOP-PD: Combination Therapy With Sertraline Plus Olanzapine Effective in the Treatment of Psychotic Depression
среда, 26 августа 2009 г.
Комбинирование клозапина с ламотриджином
Schizophrenia patients routinely are treated with polypharmacy--often with antidepressants or anticonvulsants--in attempts to improve negative symptoms, aggression, and impulsivity. Most adjuncts, however--including divalproex, antidepressants, and lithium--have shown very small, inconsistent, or no effects. The only agent with a recent meta-analysis supporting its use as augmentation in treatment-resistant schizophrenia is lamotrigine, an anticonvulsant approved for use in epilepsy...
Clozapine Augmentation with Lamotrigine
Clozapine Augmentation with Lamotrigine
воскресенье, 23 августа 2009 г.
Fatty Acid's Role in Alzheimer's Remains In Doubt
An omega-3 fatty acid (DHA) did not slow Alzheimer's, but it may help with prevention and sharpen the memories of seniors with normal age-related memory complaints.
The findings of this study "indicate that the use of 900 mg of . . . DHA per day improves learning and memory recall in healthy aging adults with mild memory complaints
Fatty Acid's Role in Alzheimer's Remains In Doubt
The findings of this study "indicate that the use of 900 mg of . . . DHA per day improves learning and memory recall in healthy aging adults with mild memory complaints
Fatty Acid's Role in Alzheimer's Remains In Doubt
вторник, 18 августа 2009 г.
нейропсихиатрические расстройства и токсоплазмоз
Toxoplasma gondii infects approximately 30% of the world's population, but causes overt clinical symptoms in only a small proportion of people. In recent years, the ability of the parasite to manipulate the behaviour of infected mice and rats and alter personality attributes of humans has been reported. Furthermore, a number of studies have now suggested T. gondii infection as a risk factor for the development of schizophrenia and depression in humans. As T. gondii forms cysts that are located in various anatomical sites including the brain during a chronic infection, it is well placed anatomically to mediate these effects directly. The T. gondii genome is known to contain 2 aromatic amino acid hydroxylases that potentially could directly affect dopamine and/or serotonin biosynthesis. However, stimulation of the immune response has also recently been associated with mood and behavioural alterations in humans, and compounds designed to alter mood, such as fluoxetine, have been demonstrated to alter aspects of immune function. Herein, the evidence for T.-gondii-induced behavioural changes relevant to schizophrenia and depression is reviewed. Potential mechanisms responsible for these changes in behaviour including the role of tryptophan metabolism and the hypothalamic-pituitary-adrenal axis are discussed. Copyright (c) 2009 S. Karger AG, Basel.
pubmed
pubmed
Миртазапин в качестве корректора акатизии вызванной антипсихотиками
OBJECTIVE: To evaluate the role of mirtazapine in the treatment of antipsychotic-induced akathisia. DATA SOURCES: MEDLINE (1966-February 2008) and PsycINFO (1967-February 2008) were searched using the terms akathisia and mirtazapine. A bibliographic search was conducted as well. STUDY SELECTION AND DATA EXTRACTION: All English-language articles identified from the search were evaluated. All primary literature was included in the review. DATA SYNTHESIS: Antipsychotic-induced akathisia can be difficult to manage and may respond to mirtazapine based on its antagonist activity at the serotonin 5-HT(2A)/5-HT(2C) receptors. Three case reports (N = 9 pts.), 1 placebo-controlled trial (N = 26), and 1 placebo- and propranolol-controlled study (N = 90) that evaluated mirtazapine for antipsychotic-induced akathisia have been published. Mirtazapine demonstrated a response rate of 53.8% compared with a 7.7% response rate for placebo, based on at least a 2-point reduction on the Barnes Akathisia Scale (global subscale; p = 0.004). Using the same criterion, mirtazapine and propranolol demonstrated efficacy based on response rates of 43.3% and 30.0% compared with placebo (6.7%; p = 0.0051). Mirtazapine was better tolerated than propranolol. In both studies, drowsiness was the most common adverse event associated with mirtazapine. CONCLUSIONS: Mirtazapine may be considered a treatment option for antipsychotic-induced akathisia. It may be especially useful for patients with contraindications or intolerability to beta-blockers and for those with comorbid depression or negative symptoms. Additional studies should be conducted to provide further evidence of mirtazapine's effectiveness in treating akathisia.
pubmed
pubmed


понедельник, 17 августа 2009 г.
A Double-blind Randomized Controlled Trial of Olanzapine Plus Sertraline vs Olanzapine Plus Placebo for Psychotic Depression
Treatment with olanzapine/sertraline was associated with higher remission rates during the trial than olanzapine/placebo (odds ratio [OR], 1.28; 95% confidence interval [CI], 1.12-1.47; P < .001); 41.9% of subjects who underwent combination therapy were in remission at their last assessment compared with 23.9% of subjects treated with monotherapy ({chi}21 = 9.53, P = .002). Combination therapy was comparably superior in both younger (OR, 1.25; 95% CI, 1.05-1.50; P = .02) and older (OR, 1.34; 95% CI, 1.09-1.66; P = .01) adults. Overall, tolerability was comparable across age groups. Both age groups had significant increases in cholesterol and triglyceride concentrations, but statistically significant increases in glucose occurred only in younger adults. Younger adults gained significantly more weight than older subjects (mean [SD], 6.5 [6.6] kg vs 3.3 [4.9] kg, P = .001).
A Double-blind Randomized Controlled Trial of Olanzapine Plus Sertraline vs Olanzapine Plus Placebo for Psychotic Depression
A Double-blind Randomized Controlled Trial of Olanzapine Plus Sertraline vs Olanzapine Plus Placebo for Psychotic Depression
вторник, 11 августа 2009 г.
Резистентные к лечению депрессии


Antidepressants can be grouped into 6 major categories: tricyclic antidepressants (TCAs), SSRIs, serotonin norepinephrine reuptake inhibitors (SNRIs), monoamine oxidase inhibitors (MAOIs), serotonin neurotransmitter (5-HT2)-receptor antagonists (eg, nefazodone, trazodone), and novel agents (eg, mirtazapine, bupropion). If a patient fails to respond to one antidepressant class, it makes sense (at least conceptually) to switch to another, although most guidelines acknowledge that 2 failed trials of SSRIs may be justifiable before switching classes.
For example, in a study by Thase and colleagues,10 58 patients failed a trial of fluoxetine; however, there was a 76% response rate to citalopram among completers. Although this study was not blinded, it is interesting that citalopram (which is believed to be the most selective of the SSRIs) was effective when another SSRI was not.
Antidepressants that are associated with discontinuation symptoms (eg, paroxetine, venlafaxine, duloxetine) may produce discontinuation syndromes when stopped that can be erroneously attributed to adverse effects of the new drug, particularly if the new drug does not possess a significant degree of serotonin reuptake inhibition.
In a study by Zarate and colleagues,21 the onset of the antidepressant effect of ketamine occurred within 2 hours. Unfortunately, the drug must be given by intravenous infusion, but because the effect persisted for 7 days, ketamine treatment may be useful if given as a series.
Another NMDA-receptor antagonist now available in the United States is memantine (FDA-approved for Alzheimer disease). Memantine was shown to be effective in an open-label study in major depression. In a double-blind, randomized trial it showed comparable effects to escitalopram in patients with major depression and alcohol dependence.
Randomized controlled trials have supported the superior efficacy of a TCA/SSRI combination, as well as a mirtazapine/SSRI combination; open studies have done the same for TCA/MAOI and SSRI/bupropion combinations.
As with lithium, a recent review concluded that the trial data that support the efficacy of T3 augmentation are of better quality with TCAs than with SSRIs
Treatment-Resistant Depression
Резистентное к лечению биполярное расстройство

In acute mania, antidepressants should be discontinued immediately. The focus should be on using evidence-based treatments for mania. Although lithium is not recommended for mixed episodes or for patients with many previous episodes, lithium and divalproex are often used before an atypical antipsychotic because they are thought to be safer with long-term use.
The most commonly recommended nonstandard treatments for treatment-resistant mania are clozapine and ECT, which have been shown to have efficacy.A combination of clozapine and ECT has also been suggested.
Several novel treatments have been studied using an augmentation approach in combination with standard treatments for treatment-resistant mania. These include donepezil, gabapentin, topiramate, mexiletine, and intravenous magnesium sulphate. The reported efficacy in these uncontrolled reports is confounded by the continuation of the previous treatments. One exception is tamoxifen, which, like lithium and valproate, inhibits protein kinase C and was found to have antimanic efficacy superior to placebo.
However, antidepressants (other than fluoxetine in combination with olanzapine) have not been shown to be efficacious in acute bipolar depression and may be associated with switching. In particular, antidepressants with norepinephrine activity including tricyclics and serotonin-norepinephrine reuptake inhibitors may have a greater risk of inducing switching than SSRIs.
For treatment-resistant acute bipolar depression, the dopaminergic agonist pramipexole and the wakefulness-promoting agent modafinil have been shown to have efficacy greater than placebo as augmentation to standard treatments.4,26 Other pharmacotherapies have been studied in uncontrolled augmentation, including donepezil, bupropion, riluzole, gabapentin, levetiracetam, and aripiprazole. Two brain-stimulating therapies—magnetic seizure therapy and repetitive transcranial magnetic stimulation (TMS)—have been studied as well.
Other approaches include augmentation with hypermetabolic thyroid supplementation, diltiazem, aripiprazole, topiramate, gabapentin, mexiletine, levetiracetam, and chromium, as well as vagus nerve stimulation. Efficacy has also been reported for levetiracetam monotherapy and a combination of topiramate and clozapine.
Treatment-Resistant Bipolar Disorder
понедельник, 10 августа 2009 г.
Синдром хронической усталости и депрессия
CFS has been linked to Epstein-Barr virus and human herpesvirus 6; however, study results have not been conclusive and the presence of these viruses does not always result in the development of CFS. Depression has been a common diagnosis, with as many as 80% of people affected with CFS misdiagnosed.
...
The majority of the scientific community now acknowledges that CFS does actually exist. While scientists have not yet identified the underlying cause of CFS or a definitive diagnostic test
Chronic Fatigue Syndrome – A Medical Mystery
...
The majority of the scientific community now acknowledges that CFS does actually exist. While scientists have not yet identified the underlying cause of CFS or a definitive diagnostic test
Chronic Fatigue Syndrome – A Medical Mystery
пятница, 24 июля 2009 г.
среда, 22 июля 2009 г.
четверг, 16 июля 2009 г.
Случаи нарушения функции печени при приёме страттеры
Reported cases of liver injury occurred within 120 days of initiation of atomoxetine in the majority of cases and some patients presented with markedly elevated liver enzymes [>20 X upper limit of normal (ULN)], and jaundice with significantly elevated bilirubin levels (>2 X ULN), followed by recovery upon atomoxetine discontinuation.
FDA
FDA
среда, 15 июля 2009 г.
диазепамовый тест
Надежным методом разграничения деперсонализации, депрессии и тревоги является диазепамовый тест (ДТ) . Он заключается в струйном (медленном) внутривенном введении раствора диазепама (седуксена). Обычная доза составляет 30 мг препарата, у пожилых и ослабленных больных иногда вводят 20 мг, при массивной деперсонализации дозу можно увеличить до 40 мг. Выделяют три основных типа ДТ. 1. Депрессивный: депрессивная симптоматика существенно не меняется, больной быстро засыпает или наступает выраженная сонливость. 2. Тревожный: быстро, часто «на игле», исчезает вся аффективная симптоматика (тревога, депрессия). Иногда наступает легкая эйфория. 3.Деперсонализационный (отставленный). В отличие от других вариантов ДТ, положительная реакция на тест наступает через 20-30 минут и выражается в исчезновении или частичной редукции деперсонализации: «все стало ярче, яснее», «появились какие-то чувства». У подавляющего большинства больных с острой деперсонализацией ДТ положительный, при хронической деперсонализации (продолжительностью многие месяцы или годы) – может выявиться неполный положительный эффект. В немногих случаях хронической деперсонализации положительная реакция на тест отсутствует. При депрессивно-деперсонализационном синдроме в нозологических рамках депрессивного расстройства возможны следующие ответы на ДТ: после редукции деперсонализации выявляется отчетливая депрессивная симптоматика или субдепрессия, иногда наступает эйфория или гипомания.
Ю.Л.Нуллер - Диагностика и терапия деперсонализационного расстройства.
Ю.Л.Нуллер - Диагностика и терапия деперсонализационного расстройства.
вторник, 14 июля 2009 г.
Антипсихотические свойства пропранолола
Propranolol in psychiatric illness.
Propranolol in chronic schizophrenia: a controlled study in neuroleptic-treated patients.
Propranolol in schizophrenia: a double blind, placebo controlled trial of propranolol as an adjunct to neuroleptic medication.
Does propranolol have an antipsychotic effect? A placebo-controlled study in acute schizophrenia.
Propranolol in chronic schizophrenia: a controlled study in neuroleptic-treated patients.
Propranolol in schizophrenia: a double blind, placebo controlled trial of propranolol as an adjunct to neuroleptic medication.
Does propranolol have an antipsychotic effect? A placebo-controlled study in acute schizophrenia.
понедельник, 13 июля 2009 г.
четверг, 9 июля 2009 г.
Treatment of Sexual Side Effects: Antidotes
Treatment of Sexual Side Effects: Antidotes
A variety of antidotes have been reported to treat SSRI-induced sexual dysfunction effectively; however, virtually all the data on these agents are derived from open case reports and case series. Insofar as sexual function improvement may be responsive to placebo effects, it is impossible to estimate the true efficacy of these antidotes.[27]
Most of these antidotes either have serotonin-blocking properties (especially 5HT-2 antagonistic effects) or augment catecholamine activity, especially that of dopamine. The antiserotonergic antidotes are cyproheptadine, buspirone, nefazodone, and mianserin. Medications enhancing dopaminergic tone include amantadine, bupropion, and stimulants, with yohimbine showing noradrenergic effects. Among the reported antidotes, the only 2 without antiserotonergic effects or catecholaminergic activity are gingko biloba and urecholine.
Cyproheptadine is an antihistamine with antiserotonergic properties that has been reported for over a decade to reverse antidepressant-induced sexual dysfunction. Only case reports and case series attest to its efficacy.[13,42-44] Effective doses range from 2mg to 16mg. In the most recent and largest case series, 12 of 25 patients described improvement in sexual function when treated with cyproheptadine (mean dose, 8.6mg).[13] Anorgasmia is the sexual side effect most often reported to be alleviated by cyproheptadine. Cyproheptadine is effective when taken either on an as-needed basis (typically, 1 to 2 hours before intercourse) or on a regular basis.
However, cyproheptadine's utility is often limited by its potential side effects. Excessive sedation and the reversal of the therapeutic effect of the antidepressant are major problems that limit its usefulness. Effectively treated depression and bulimic symptoms have been reported to reemerge soon after cyproheptadine was started.[42,45-48] This reversal of therapeutic effects is itself reversible upon discontinuation.
Buspirone is a serotonin-IA partial agonist typically prescribed to treat persistent anxiety. One case series reported that buspirone reversed both decreased sexual interest and orgasmic dysfunction caused by SSRIs.[49] Most patients using buspirone to treat sexual dysfunction take it daily. The dosage is the same as that used for anxiety (15mg to 60mg daily). The mechanism of action of buspirone in treating sexual dysfunction may be reduction of serotonergic tone via stimulation of presynaptic autoreceptors or the alpha-2 antagonist effects of one of buspirone's major metabolites, 1-pyrimidinylpiperazine.
Nefazodone and mianserin are antidepressants with strong postsynaptic blocking properties. In one case report, nefazodone 150mg taken 1 hour prior to sexual activity completely reversed sertraline-induced anorgasmia.[50] Mianserin, an antidepressant with 5HT-2 and alpha-2 adrenergic antagonist properties, is available in many countries but not in the US. It has been reported to reverse serotonin reuptake inhibitor-induced sexual dysfunction in 9 of 15 patients.[51] Mirtazapine is similar in its biological activity to mianserin and might also be effective in reversing sexual side effects. No case reports or case series have yet been published attesting to this, although clinicians have described such an effect. The putative capacity of mianserin and mirtazapine to reverse sexual side effects can be attributed either to their serotonergic activity or presynaptic alpha-2 activity.
Amantadine, a dopamine agonist, is used both as an antiviral agent and as a treatment for Parkinson's disease. It has been shown in a number of small case series to reverse anorgasmia.[13,52-54] Reported effective doses have ranged between 100mg to 400mg taken either on a daily or as-needed basis. In the most recent case series, 8 (42%) out of 19 patients with SSRI-induced sexual dysfunction improved with amantadine 200mg daily.[13] Given dopamine's consistent effect as a neurotransmitter involved in sexual arousal, a number of other dopamine agonists have been explored as treatments for sexual side effects.[2,55,56]
Bupropion is another commonly touted antidote for SSRI-induced sexual dysfunction.[57,58] It is assumed that the mechanism of action by which bupropion reverses sexual side effects is its weak dopamine agonism. The evidence for bupropion's efficacy is scant, except for unpublished, anecdotal reports, one case report,[57] and a case series[58] in which 31 (66%) of 47 patients showed improvement when bupropion was added to the regimen along with the serotonergic antidepressant. Most patients (18/31) with a successful outcome responded to as-needed use of bupropion 75mg to 150mg. Libido, arousal, and orgasmic difficulties were all effectively reversed. Fifteen percent of treated patients stopped taking bupropion because of its stimulation side effects. It is unclear whether bupropion doses need to be somewhat lower than usual when added to fluoxetine or paroxetine, to compensate for pharmacokinetic interactions resulting in increased bupropion levels.[59]
Stimulants, such as methylphenidate, D-amphetamine, and pemoline, are reported to reverse a variety of sexual side effects caused by SSRIs or MAOIs.[60-62] Low doses of 10mg-25mg of methylphenidate or D-amphetamine have been effective. One should add stimulants to an MAOI with extreme caution because of the risk of a hypertensive episode. However, use of an MAOI/stimulant combination has been shown to be safe in a case series.[63] SSRI/stimulant combinations show no similar risks.
Yohimbine is available with or without a prescription (and with unclear purity) in health food stores. It is an alkaloid from the bark of Corynanthe yohimbi (family, Rubiaceae) and has been used for decades to reverse erectile dysfunction.[64-66] Its efficacy in treating sexual dysfunction may be associated with its ability to block presynaptic alpha-2 adrenergic sites, leading to enhanced adrenergic tone.[65] A variety of sexual side effects have been reported to be alleviated by yohimbine in doses ranging from 2.7mg to 16.2mg daily, prescribed either on a regular 5.4mg 3 times daily basis or on an as-needed basis with single doses up to 16.2mg.[13,67-69] In the largest case series, 17 (81%) of 21 patients showed improvement of sexual side effects when treated with yohimbine (mean dose, 16.2mg).[12]
Typical side effects associated with yohimbine include anxiety, nausea, flushing, urinary urgency, and sweating. Yohimbine has been the subject of the only double-blind, placebo-controlled study to evaluate treatment of sexual dysfunction occurring as a drug side effect.[27] Unfortunately, the placebo effect was marked, showing a minimal drug-placebo difference with yohimbine given at a dose of 5.4mg 3 times daily. Yohimbine is also available in lower potency without a prescription. The purity, potency, and safety of these preparations, however, are unknown.
Bethanechol is a cholinergic agonist that has occasionally been useful in reversing sexual dysfunction associated with TCAs and MAOIs.[70-73] Typical doses are 10mg to 20mg as needed or 30mg to 100mg daily in a divided dose. Potential side effects with bethanechol include diarrhea, cramps, and diaphoresis. No reports have evaluated or suggested the efficacy of bethanechol for treating SSRI-induced sexual side effects.
Gingko biloba is an herbal extract reported to reverse a variety of sexual dysfunctions associated with antidepressants. Information about gingko's ability in this regard is derived from the experience of 1 clinician presenting a large case series.[74] The response rate was greater than 80%, with doses ranging from 60mg twice daily to 120mg twice daily (mean daily dose, 207mg). Reported side effects include gastrointestinal upset, lightheadedness, and stimulation effects. Because gingko may inhibit platelet-activating factor, caution should be used in considering its use by any patient with a bleeding diathesis. The mechanism by which gingko might alleviate sexual dysfunction is unknown.
http://www.medscape.com/viewarticle/430614_5
A variety of antidotes have been reported to treat SSRI-induced sexual dysfunction effectively; however, virtually all the data on these agents are derived from open case reports and case series. Insofar as sexual function improvement may be responsive to placebo effects, it is impossible to estimate the true efficacy of these antidotes.[27]
Most of these antidotes either have serotonin-blocking properties (especially 5HT-2 antagonistic effects) or augment catecholamine activity, especially that of dopamine. The antiserotonergic antidotes are cyproheptadine, buspirone, nefazodone, and mianserin. Medications enhancing dopaminergic tone include amantadine, bupropion, and stimulants, with yohimbine showing noradrenergic effects. Among the reported antidotes, the only 2 without antiserotonergic effects or catecholaminergic activity are gingko biloba and urecholine.
Cyproheptadine is an antihistamine with antiserotonergic properties that has been reported for over a decade to reverse antidepressant-induced sexual dysfunction. Only case reports and case series attest to its efficacy.[13,42-44] Effective doses range from 2mg to 16mg. In the most recent and largest case series, 12 of 25 patients described improvement in sexual function when treated with cyproheptadine (mean dose, 8.6mg).[13] Anorgasmia is the sexual side effect most often reported to be alleviated by cyproheptadine. Cyproheptadine is effective when taken either on an as-needed basis (typically, 1 to 2 hours before intercourse) or on a regular basis.
However, cyproheptadine's utility is often limited by its potential side effects. Excessive sedation and the reversal of the therapeutic effect of the antidepressant are major problems that limit its usefulness. Effectively treated depression and bulimic symptoms have been reported to reemerge soon after cyproheptadine was started.[42,45-48] This reversal of therapeutic effects is itself reversible upon discontinuation.
Buspirone is a serotonin-IA partial agonist typically prescribed to treat persistent anxiety. One case series reported that buspirone reversed both decreased sexual interest and orgasmic dysfunction caused by SSRIs.[49] Most patients using buspirone to treat sexual dysfunction take it daily. The dosage is the same as that used for anxiety (15mg to 60mg daily). The mechanism of action of buspirone in treating sexual dysfunction may be reduction of serotonergic tone via stimulation of presynaptic autoreceptors or the alpha-2 antagonist effects of one of buspirone's major metabolites, 1-pyrimidinylpiperazine.
Nefazodone and mianserin are antidepressants with strong postsynaptic blocking properties. In one case report, nefazodone 150mg taken 1 hour prior to sexual activity completely reversed sertraline-induced anorgasmia.[50] Mianserin, an antidepressant with 5HT-2 and alpha-2 adrenergic antagonist properties, is available in many countries but not in the US. It has been reported to reverse serotonin reuptake inhibitor-induced sexual dysfunction in 9 of 15 patients.[51] Mirtazapine is similar in its biological activity to mianserin and might also be effective in reversing sexual side effects. No case reports or case series have yet been published attesting to this, although clinicians have described such an effect. The putative capacity of mianserin and mirtazapine to reverse sexual side effects can be attributed either to their serotonergic activity or presynaptic alpha-2 activity.
Amantadine, a dopamine agonist, is used both as an antiviral agent and as a treatment for Parkinson's disease. It has been shown in a number of small case series to reverse anorgasmia.[13,52-54] Reported effective doses have ranged between 100mg to 400mg taken either on a daily or as-needed basis. In the most recent case series, 8 (42%) out of 19 patients with SSRI-induced sexual dysfunction improved with amantadine 200mg daily.[13] Given dopamine's consistent effect as a neurotransmitter involved in sexual arousal, a number of other dopamine agonists have been explored as treatments for sexual side effects.[2,55,56]
Bupropion is another commonly touted antidote for SSRI-induced sexual dysfunction.[57,58] It is assumed that the mechanism of action by which bupropion reverses sexual side effects is its weak dopamine agonism. The evidence for bupropion's efficacy is scant, except for unpublished, anecdotal reports, one case report,[57] and a case series[58] in which 31 (66%) of 47 patients showed improvement when bupropion was added to the regimen along with the serotonergic antidepressant. Most patients (18/31) with a successful outcome responded to as-needed use of bupropion 75mg to 150mg. Libido, arousal, and orgasmic difficulties were all effectively reversed. Fifteen percent of treated patients stopped taking bupropion because of its stimulation side effects. It is unclear whether bupropion doses need to be somewhat lower than usual when added to fluoxetine or paroxetine, to compensate for pharmacokinetic interactions resulting in increased bupropion levels.[59]
Stimulants, such as methylphenidate, D-amphetamine, and pemoline, are reported to reverse a variety of sexual side effects caused by SSRIs or MAOIs.[60-62] Low doses of 10mg-25mg of methylphenidate or D-amphetamine have been effective. One should add stimulants to an MAOI with extreme caution because of the risk of a hypertensive episode. However, use of an MAOI/stimulant combination has been shown to be safe in a case series.[63] SSRI/stimulant combinations show no similar risks.
Yohimbine is available with or without a prescription (and with unclear purity) in health food stores. It is an alkaloid from the bark of Corynanthe yohimbi (family, Rubiaceae) and has been used for decades to reverse erectile dysfunction.[64-66] Its efficacy in treating sexual dysfunction may be associated with its ability to block presynaptic alpha-2 adrenergic sites, leading to enhanced adrenergic tone.[65] A variety of sexual side effects have been reported to be alleviated by yohimbine in doses ranging from 2.7mg to 16.2mg daily, prescribed either on a regular 5.4mg 3 times daily basis or on an as-needed basis with single doses up to 16.2mg.[13,67-69] In the largest case series, 17 (81%) of 21 patients showed improvement of sexual side effects when treated with yohimbine (mean dose, 16.2mg).[12]
Typical side effects associated with yohimbine include anxiety, nausea, flushing, urinary urgency, and sweating. Yohimbine has been the subject of the only double-blind, placebo-controlled study to evaluate treatment of sexual dysfunction occurring as a drug side effect.[27] Unfortunately, the placebo effect was marked, showing a minimal drug-placebo difference with yohimbine given at a dose of 5.4mg 3 times daily. Yohimbine is also available in lower potency without a prescription. The purity, potency, and safety of these preparations, however, are unknown.
Bethanechol is a cholinergic agonist that has occasionally been useful in reversing sexual dysfunction associated with TCAs and MAOIs.[70-73] Typical doses are 10mg to 20mg as needed or 30mg to 100mg daily in a divided dose. Potential side effects with bethanechol include diarrhea, cramps, and diaphoresis. No reports have evaluated or suggested the efficacy of bethanechol for treating SSRI-induced sexual side effects.
Gingko biloba is an herbal extract reported to reverse a variety of sexual dysfunctions associated with antidepressants. Information about gingko's ability in this regard is derived from the experience of 1 clinician presenting a large case series.[74] The response rate was greater than 80%, with doses ranging from 60mg twice daily to 120mg twice daily (mean daily dose, 207mg). Reported side effects include gastrointestinal upset, lightheadedness, and stimulation effects. Because gingko may inhibit platelet-activating factor, caution should be used in considering its use by any patient with a bleeding diathesis. The mechanism by which gingko might alleviate sexual dysfunction is unknown.
http://www.medscape.com/viewarticle/430614_5
среда, 8 июля 2009 г.
ацетилцистеин и трихотилломания
Группе из 50 человек, страдающих трихотилломанией, предложили принять участие в 12-недельном исследовании, в котором половине из них давали таблетки, содержащие аминокислоту N-ацетилцистеин, а остальным — плацебо. Оказалось, спустя 12 недель, что среди людей, принимавших аминокислоты, значительно ослабла мания выдергивать у себя волосы, по сравнению с контрольной группой, сообщили специалисты.
Прием ацетилцистеина может уменьшать симптомы трихотилломании
Прием ацетилцистеина может уменьшать симптомы трихотилломании
вторник, 7 июля 2009 г.
четверг, 2 июля 2009 г.
Сравнение окскарбазепина и карбамазепина в терапии аффективных расстройств
In summary, the patient charts reviewed demonstrated that carbamazepine, as well as, oxcarbazepine are equally effective and tolerable as mood stabilizers.
Effectiveness and Tolerability of Carbamazepine vs. Oxcarbazepine as Mood Stabilizers
Effectiveness and Tolerability of Carbamazepine vs. Oxcarbazepine as Mood Stabilizers
Психоз после приёма валацикловира
METHOD: The patient presented with irritable mood and grandiose delusions 72 hours after starting valacyclovir for genital herpes. Valacyclovir treatment was stopped, and risperidone was initiated. RESULTS: The symptoms continued after stopping the valacyclovir, but improved with risperidone. DISCUSSION:There are reports of neuropsychiatric side effects with valacyclovir’s structural analogs in elderly patients with renal dysfunction. Clinicians should be aware that valacyclovir may induce psychosis with manic presentation in young, healthy patients without a psychiatric history.
Case Report
Case Report
Кататония при отмене клоназепама
BACKGROUND: Catatonia is a often a complex syndrome. It has been divided into categories of simple and malignant, with the latter being a more severe form involving autonomic instability and/or fever and having a higher mortality rate. OBJECTIVE: There have been only two cases presented in the literature postulating benzodiazepine-withdrawal as a possible trigger for malignant catatonia. Here, the authors present a case of catatonia likely caused by abrupt benzodiazepine discontinuation; they also discuss neurobiological mechanisms relating to catatonia. METHOD: The authors report on a 60-year-old man with a history of depression and posttraumatic stress disorder who was brought to the emergency department with acute confusion, grimacing, stereotypy, refusal of food and water, muscle rigidity, mutism, and extreme negativism. He had recently and abruptly discontinued all psychotropic medication. RESULTS: After administration of lorazapam, the patient was re-started on clonazepam, after which there was a complete and sustained resolution of catatonic symptoms and autonomic instability. CONCLUSION: Catatonia may result from a wide variety of etiologies. Catatonia due to benzodiazepine-withdrawal is a rare but serious condition that may be difficult to distinguish from other causes of catatonia. The mechanism by which catatonia may be precipitated by benzodiazepine-withdrawal is unknown, but likely involves a rapid decrease in GABA transmission in the central nervous system.
Case Report
Case Report
Антидепрессанты короткого действия в терапии БАР с быстрой сменой фаз
"I have found that in bipolar patients with extreme diurnal variation of mood (characterized by severe a.m.-hour depression followed by significant brightening in the evening), the non-time-release preparations of medications, such as bupropion and venlafaxine, given in low doses in the a.m. hours only can be very helpful and less likely to cause manic switching. Conversely, the long-acting preparations of the same medications tend to cause a reversal of diurnal variation, with improvement in the a.m. hours and agitation in the p.m. hours. It might turn out that short half-life reuptake inhibitors have a place in treating bipolar depression. Other relatively short-acting agents, such as atomoxetine, may also fall into this category."
The Use of Short Half-Life Antidepressants in the Treatment of Bipolar Depression
The Use of Short Half-Life Antidepressants in the Treatment of Bipolar Depression

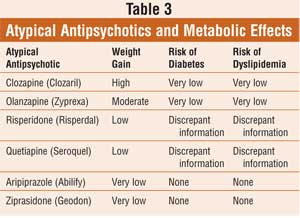
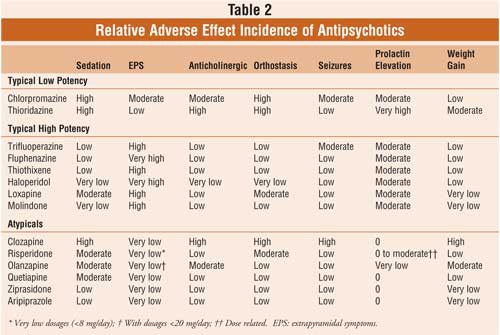

Подписаться на:
Сообщения (Atom)